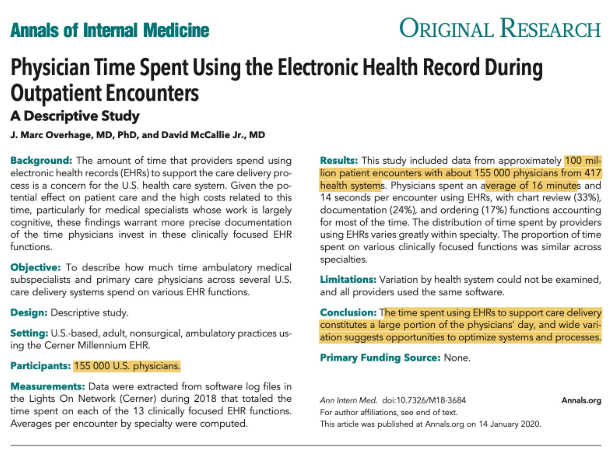
Link to full PDF: ACG Clinical Guideline: Small Intestinal Bacterial Overgrowth
M Pimentel et al. Am J Gastroenterol 2020;00:1–14. https://doi.org/10.14309/ ajg.0000000000000501; published online January 8, 2020
One key point is that the authors acknowledge that almost all of their recommendations are based on a very low level of evidence. In fact, only one of their 6 recommendations in Table 1 is considered to have more evidence and it is rated as low level of evidence.
The article provides an in-depth review of small intestinal bacterial overgrowth including underlying homeostasis mechanisms/pathophysiology (Tables 3 & 4) and treatments. For those needing treatment, the authors list options in Table 5 including rifaximin, amoxicillin-clavulanic acid, ciprofloxacin, doxycycline, metronidazole, neomycin, norfloxacin, tetracycline, and trimethoprim-sulfamethoxazole.
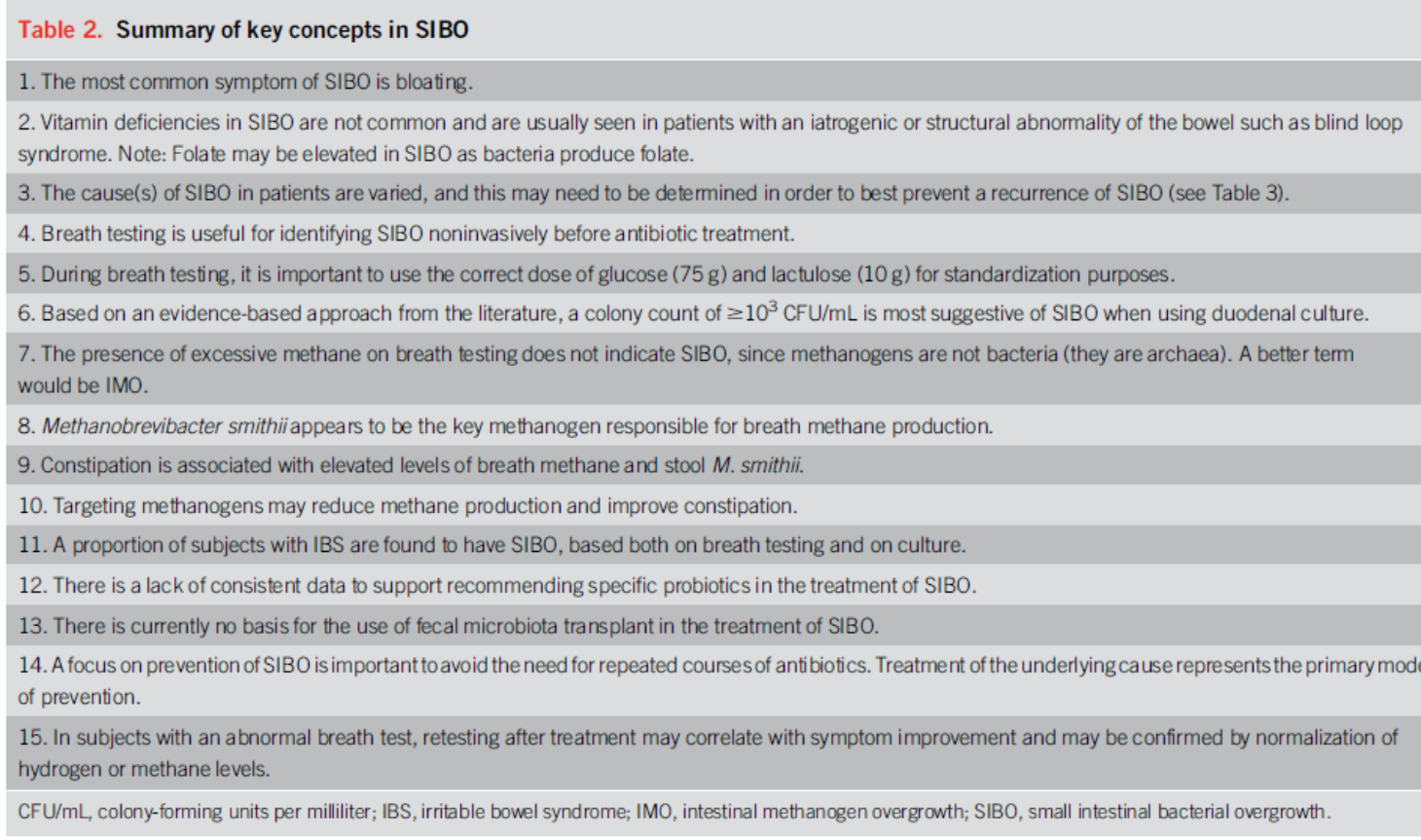
Image Available from Lizzie Aby Feed
Related blog posts:
- NASPGHAN#19 Intestinal Failure Session (Part 2)
- Breath Testing for Bacterial Overgrowth. Review with recommendations on how to perform breath testing properly
- Breath Test Reliability for Bacterial Overgrowth
- Expert Advice on Bloating
- Mechanisms of irritable bowel syndrome
- What is the risk with Rifaximin? | gutsandgrowth
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.