Link to Abbott website: Facts for Parents About Heavy Metals and Infant Formula
Some excepts:
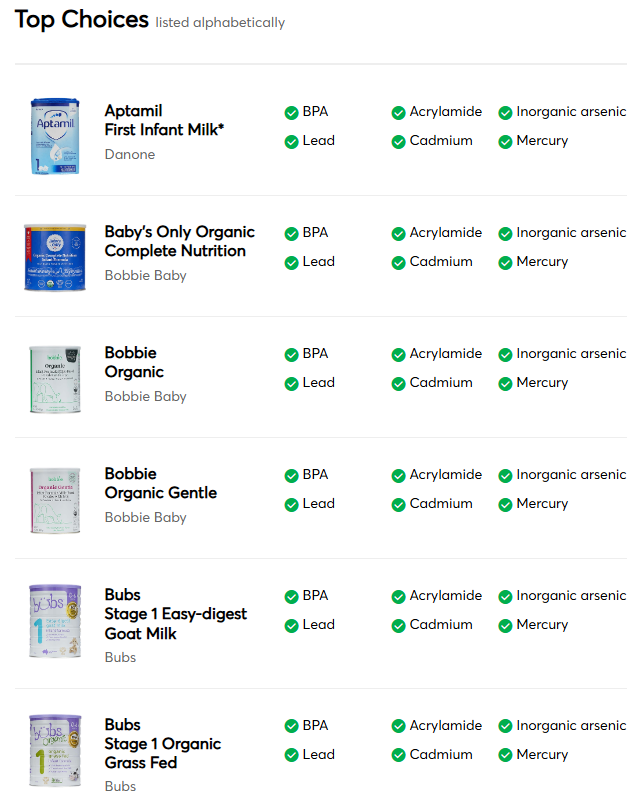
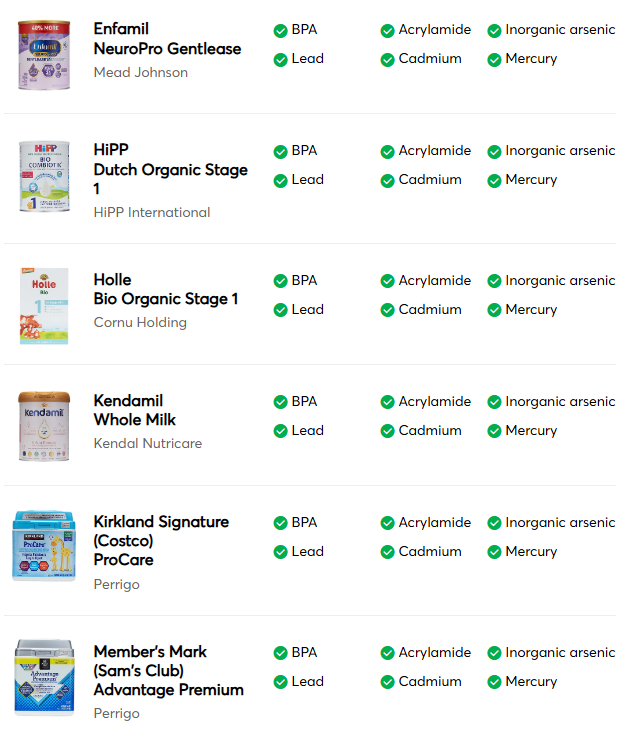
Consumer Reports published a report on the levels of heavy metals in U.S. infant formulas. In response, we want to share some important information with parents regarding the report.
- First and foremost, Abbott’s Similac infant formulas are safe, and parents can use them confidently.
- The results reported by Consumer Reports for our infant formulas meet the regulations for heavy metals already set by the European Commission and Health Canada. FDA is currently developing limits for infant formula in the U.S.
- Abbott has a multi-step quality process for heavy metals to ensure that levels are below the relevant regulatory requirements in the countries we serve.
Occurrence of Heavy Metals
Heavy metals are naturally occurring in the environment, including in the soil, water, or air where foods are grown. As a result, they are present in low levels in almost anything we eat or drink, including in baby food, all brands of infant formula, fruits and vegetables, and human breast milk.
Commitment to Safety and Quality…
The levels of heavy metals that Consumer Reports detected in Abbott’s formulas are very low—just a few parts per billion. To put that in perspective, a single ppb equals a single grain of sand in 730 pounds of sand.
Approach to Heavy Metals…
Individual ingredients that we believe may contain trace heavy metals (due to absorption from the natural environment) are tested during the qualification process before we approve them for use in our products. We also have an ongoing surveillance testing program after the qualification process designed to periodically test samples of ingredients and finished products to ensure that our supplier and ingredient qualification process is working as intended...Parents can continue to use them with confidence.
Related blog posts:
- Safe Baby Formula Choices Based on Consumer Reports Testing
- Advice on Arsenic in Baby Foods (levels are higher in rice cereal than in formulas)
- Arsenic in Rice –New Recommendations