I am a pediatric gastroenterologist at GI Care for Kids (previously called CCDHC) in Atlanta, Georgia. The goal of my blog is to share some of my reading in my field more broadly. In addition, I wanted to provide my voice to a wide range of topics that often have inaccurate or incomplete information.
Before starting this blog in 2011, I would tear out articles from journals and/or keep notes in a palm pilot. This blog helps provide an updated source of information that is easy to access and search, along with links to useful multimedia sources.
I was born and raised in Chattanooga. After graduating from the University of Virginia, I attended Baylor College of Medicine. I completed residency and fellowship training at the University of Cincinnati at the Children’s Hospital Medical Center. I received funding from the National Institutes of Health for molecular biology research of the gastrointestinal tract.
During my fellowship, I had the opportunity to work with some of the most amazing pediatric gastroenterologists and mentors. Some of these individuals included Mitchell Cohen, William Balistreri, James Heubi, Jorge Bezerra, Colin Rudolph, John Bucuvalas, and Michael Farrell. I am grateful for their teaching and their friendship. During my training with their help, I received a nationwide award for the best research by a GI fellow.
I have authored numerous publications/presentations including original research, case reports, review articles, and textbook chapters on various pediatric gastrointestinal problems. In addition, I have been recognized by Atlanta Magazine as a "Top Doctor" in my field multiple times.
Currently, I am the vice chair of the section of nutrition for the Georgia Chapter of the American Academy of Pediatrics. In addition, I am an adjunct Associate Clinical Professor of Pediatrics at Emory University School of Medicine. Other society memberships have included the North American Society for Pediatric Gastroenterology Hepatology and Nutrition (NASPGHAN), American Academy of Pediatrics, the Food Allergy Network, the American Gastroenterology Association, the American Association for the Study of Liver Diseases, and the Crohn’s and Colitis Foundation.
As part of a national pediatric GI organization called NASPGHAN (and its affiliated website GIKids), I have helped develop educational materials on a wide-range of gastrointestinal and liver diseases which are used across the country. Also, I have been an invited speaker for national campaigns to improve the evaluation and treatment of gastroesophageal reflux disease, celiac disease, eosinophilic esophagitis, hepatitis C, and inflammatory bowel disease (IBD). Some information on these topics has been posted at my work website, www.gicareforkids.com, which has links to multiple other useful resources.
I am fortunate to work at GI Care For Kids. Our group has 17 terrific physicians with a wide range of subspecialization, including liver diseases, feeding disorders, eosinophilic diseases, inflammatory bowel disease, cystic fibrosis, DiGeorge/22q, celiac disease, and motility disorders. Many of our physicians are recognized nationally for their achievements. Our group of physicians have worked closely together for many years. None of the physicians in our group have ever left to join other groups. I have also worked with the same nurse (Bernadette) since I moved to Atlanta in 1997.
For many families, more practical matters about our office include the following:
– 14 office/satellite locations
– physicians who speak Spanish
– cutting edge research
– on-site nutritionists
– on-site psychology support for abdominal pain and feeding disorders
– participation in ImproveCareNow to better the outcomes for children with inflammatory bowel disease
– office endoscopy suite (lower costs and easier scheduling)
– office infusion center (lower costs and easier for families)
– easy access to nursing advice (each physician has at least one nurse)
I am married and have two sons (both adults). I like to read, walk/hike, bike, swim, and play tennis with my free time.
I do not have any financial relationships with pharmaceutical companies or other financial relationships to disclose. I have helped enroll patients in industry-sponsored research studies.
Patients with CP are at risk for macro- and micronutrient deficiencies. Patients should be monitored for growth and pubertal devolvement, dietary intake, and fat-soluble vitamin deficiencies. Growth and dietary intake should be reviewed at every clinic visit, a minimum of every 6 to 12 months. Fat-soluble vitamin laboratory analysis should occur every 12 to 18 months or as clinically indicated. (Grade 1B)
There is a clear role for PERT in children with CP who have EPI with steatorrhea, poor growth and/or nutritional deficiencies. PERT dosing for CP associated EPI (see Table 1) is similar to that used in patients with CF. (Grade 1B). EPI screening can be done with stool elastase (Figure 1).
Screen yearly with HbA1c level (GRADE 1C). OGTT should be performed annually once a patient is considered to have pre-diabetes. (GRADE 1C)
Insufficient data exists to recommend the use of antioxidants as a treatment to prevent EPI or other disease progression in children with CP. (GRADE 2C)
There is insufficient data to recommend PERT as therapy for pain in children without EPI. (GRADE 1B); there is insufficient data to recommend antioxidants, steroids, leukotriene antagonists, or somatostatins in the management of pain for children with CP. (GRADE 2C)
Recommends advising patients to avoid alcohol abuse and smoking
The majority of pancreatic fluid collections will resolve spontaneously with supportive care. Intervention is reserved for complications from mass-effect, infection/necrosis or if spontaneous regression of the collection is thought to be unlikely. (GRADE 1B)
Steven Liu for Epic functionality (in the ~first 20 minutes)
John Pohl for Cerner functionality (in the ~second 20 minutes)
Jennifer Lee discussed patient portal, improving provider-patient communication, & protecting adolescent confidentiality-21st Century Cures Act
Jeannie Huang discussed the role of EHRs in value-based health care and clinical data collection.
Since our group mainly uses Epic, I will summarize some of the tips from Steven Liu, who also is our group’s Epic Physician Champion. Anyone who listened to the webinar will realize how there are so many tricks available. Some of the material from the talk is at the bottom in the form of screenshots; however, much of the information in the webinar is proprietary to EPIC and cannot be shared without permission.
Here are some of the key points:
Customize your templates for progress notes/H&Ps/other notes.
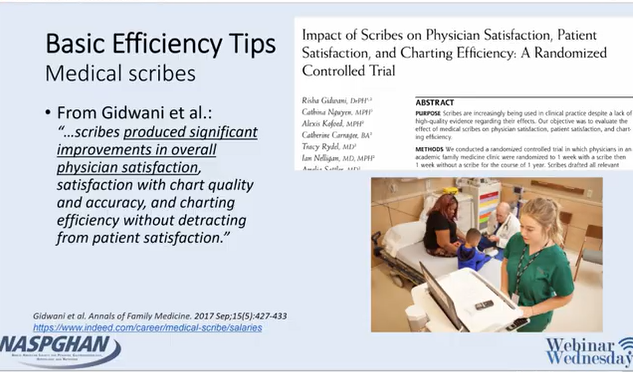
Scribes may relieve frustration and be a good investment
Use Smartphrases and Smartlinks
Smartphrases can be taken (or customized) from other users -can browse your superusers phrases by looking under Smartphrase manager
Smartforms can be very useful (eg. ImproveCareNow)
Using Dictionary, users can change autocorrect: example: if you type EoE, you could have it modified to Eosinophilic Esophagitis
Utilize customized filters (wrench icon) under the chart review tabs
Take advantage of the Chart Search function
can search “PPI” or “calprotectin” and this will identify if patient has used a PPI or had a calprotectin
can access this feature quickly with CTRL-spacebar
Shortcuts can save time -examples ALT-A and ALT-S
Take the time to build customized order panels, like “Celiac Annual Labs”
Health Maintenance Checklists can be incorporated but users may need their system to activate this feature
There is an Inbox Reminder function (to remind patient to get an appointment or test) or you can send a inbox message to yourself with a future date
For more sophisticated users: generating reports with Workbench
Epic has free classes (User Web -see slide below) available to help practitioners become more proficient (eg. Power User Course)
My take: Steven has helped everyone in our practice & listening to his talk makes me realize that I need to learn a good bit more and take some of his stuff. This EHR webinar provides a lot of tips to help good EHR users become better users. For those interested in research, understanding EHRs will be crucial going forward.
“Due to their mechanism of action, both mRNA COVID-19 vaccines are recommended for all patients with CLD (compensated or decompensated) and immunosuppressed SOT recipients.”
“The AASLD recommends that providers advocate for prioritizing patients with compensated or decompensated cirrhosis or liver cancer, patients receiving immunosuppression such as SOT recipients, and living liver donors for COVID-19 vaccination based upon local health policies, protocols, and vaccine availability.”
Associate Director, Emory Global Health Institute Director, Global Health Office of Pediatrics Professor of Global Health, Rollins School of Public Health Professor of Pediatrics, Emory University School of Medicine
BRINDA: BIOMARKERS REFLECTING INFLAMMATION AND NUTRITIONAL DETERMINANTS OF ANEMIA
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition
JF Ludvigsson et al NEJM 2021; 384: 669-671. Full text: Open Schools, Covid-19, and Child and Teacher Morbidity in Sweden In this letter to the editor, the authors report on outcomes in Sweden, which kept schools open during the pandemic; time period: from March 1-June 30, 2020 (schools end around June 10th). Key findings:
Among 1-16 years of age (~1.95 million in total), 15 required ICU admission; there were no deaths in this age group
“Fewer than 10 pre-school teachers [1-6 years] and 20 schoolteachers received ICU care up to June 30, 2020.” Excluding health care workers, the occupational risk was similar to other occupations, with relative risk of 1.10 (0.49-2.49, 95% CI) and 0.43 (0.28-0.68, 95% CI) for preschool and school teachers respectively.
My take: This study suggests that school teachers are at similar risk for COVID-19 infection as other essential workers. In Sweden, during this timeframe, distancing but not masking was recommended. Thus, transmission rates could be lowered further.
The authors utilized three databases for children aged 2 months to 18 years: Medicaid Databases from Arizona (2009-2017) and Wisconsin (2005-2014) (public insurance databases) and The Truven Health Analytics MarketScan Commercial Claims and Encounters Database (2009-2015) (a nationwide private insurance database).
Key findings:
There were 126 002 and 367 256 children 5 years of age or younger with pediatric feeding disorders (PFD) with public and private insurance, respectively
In 2014, the annual prevalence of PFD was 1 in 23, 1 in 24, and 1 in 37 in children under 5 years in the publicly insured cohorts in Wisconsin, Arizona, and the privately insured cohort, respectively.
The prevalence of PFD in children <5 years (range: 27-44 per 1000 children) exceeds the prevalence of U.S. children with autism spectrum disorder (~17 per 1000 children at age 8 year) and eating disorders like anorexia nervosa and bulimia (8 and 13 per 100,000 persons per year).
In an associated editorial (pg 13-14), Rachel Rosen notes that “despite their high prevalence, the lack of studies funded by the National Institutes of Health…is striking.”
My take: This study provides useful data on PFD prevalence. PFD have a wide range of associated diseases, including prematurity, neurologic disorders/developmental delay, congenital heart disease, chronic lung disease, autism, and congenital bowel disorders. In some, PFD are related to poorly-understood feeding aversions.
After the start of immunosuppressive therapy, bilirubin, albumin, and INR normalized in 70%, 77%, and 69%, respectively, in a median of 2.6 months, 3 months, and 4 weeks, respectively, in patients with A-AIH and AS-AIH
Deterioration of liver function (bilirubin, INR) after 2 weeks of treatment should lead to rapid evaluation for LT and consideration of second-line medication.
The cumulative incidence of waitlist mortality was 5.2%. Median waitlist time was 83 days.
In multivariable analysis (n = 2253), increasing bilirubin level ( P < .001), portal vein thrombosis ( P = .03), and ventilator dependence ( P < .001) at listing were associated with a higher risk, whereas weight ≥10 kg at listing ( P = .009) was associated with a lower risk of waitlist mortality.
In The Shawshank Redemption, Andy Dufresne (Tim Robbins) manages to escape prison by crawling through 500 yards of a filthy sewage pipe. It seems like a similar effort will be needed to find out how to benefit from fecal transplantation when given for problems like irritable bowel syndrome and metabolic disease/obesity. Some recent studies and associated editorials are noted below.
Key finding: At week 12, 56% of patients given donor stool reported improvement in both primary endpoints compared with 26% of patients given placebo (P = .03).
This editorial stresses that trials of FMT in IBS have had inconsistent results and risks are unclear. “How many clinicians inform patients receiving FMT that the donor microbiota might include components that increase (or decrease) one’s risk of colorectal cancer?” Part of the problem is “due, in part, because a normal microbiome has not been defined.”
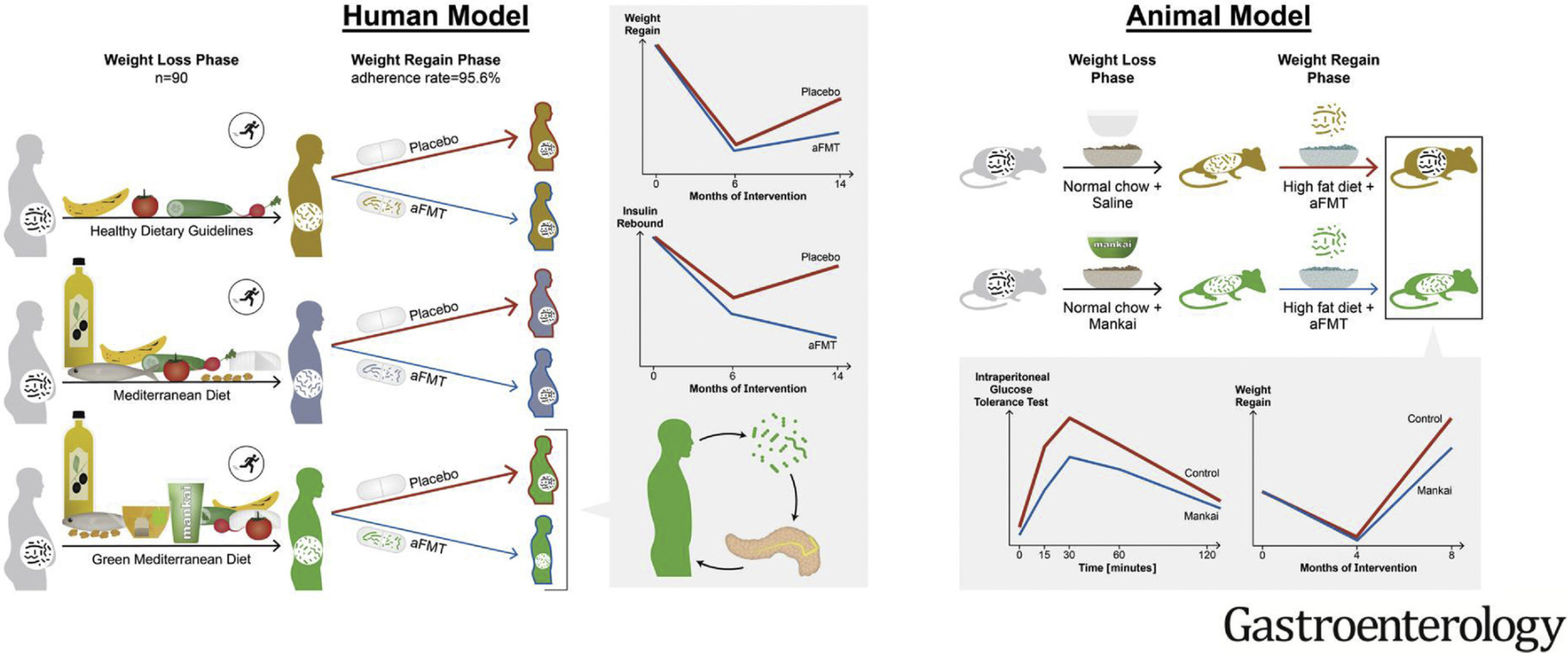
In this randomized controlled trial with 90 participants, autologous FMT (aFMT) significantly attenuated weight regain in the green-Mediterranean group (aFMT, 17.1%, vs placebo, 50%; P = .02) and improved insulin resistance: insulin rebound (aFMT, –1.46 ± 3.6 μIU/mL vs placebo, 1.64 ± 4.7 μIU/mL; P = .04) (Graphical abstract below)
In mice, Mankai-modulated aFMT in the weight-loss phase compared with control diet aFMT, significantly prevented weight regain and resulted in better glucose tolerance during a high-fat diet–induced regain phase (all, P < .05).
“These findings add support to the current body of evidence that the gut microbiota have a role in weight gain and metabolism. However, many questions remain. Indeed, although studies have shown varying degrees of effectiveness of FMT in the improvement of metabolic parameters in human participants, there has been no evidence yet that FMT can induce weight loss in obese patients.”
“The finding that maintenance of weight loss was only seen in the one dietary group consuming the Mediterranean diet plus green tea and Mankai supplement who received autologous FMT, would suggest that specific microbial profiles may be involved and that weight loss per se may not result in the required microbial profiles.”
Figure 1 from editorial: Challenges associated with the use of fecal microbial transplantation (FMT) as treatment
My take: Both of these studies show that modulation of the fecal microbiome may be helpful under the right set of circumstances to help with both irritable bowel syndrome and metabolic syndrome. However, ‘hundreds of yards’ of more research is needed to determine if this is really feasible and to assure that the benefits outweigh the potential risks.
“On November 25, 2020, … the U.S. Supreme Court, by a 5-to-4 vote, undermined states’ ability to control that pandemic.” (Roman Catholic Diocese of Brooklyn v. Cuomo)
Initially, most courts rejected challenges to restrictions imposed by governors during the pandemic. “Initially, most courts rejected these claims, citing the Supreme Court’s 1905 decision in Jacobson v. Massachusetts, which upheld a Cambridge, Massachusetts, regulation mandating smallpox vaccination during an outbreak.”
After the appointment of Justice Amy Coney Barrett, ” there was now a 5-to-4 majority willing to block limits on religious services.” This was based on the rationale that it is unlawful to “single out houses of worship for especially harsh treatment” and that “even in a pandemic, the Constitution cannot be put away and forgotten.”
In dissent, “Justice Stephen Breyer pointed to epidemiologic evidence that in-person worship may pose a greater risk than shopping and other activities that were less stringently regulated to argue that the Court should defer to state officials.”
“The Court’s eagerness to intervene even though New York’s orders were no longer in effect and its failure to consider epidemiologic evidence in determining which activities are comparable to worship will serve as a warning” against “state orders that impose tighter measures on worship…[and] suggests that states will not be able to act before super-spreader events occur or as long as other states take a more lax approach.”
The author note that “although courts should not abdicate their role during a pandemic, they also should not rush to assume an expertise they lack.”
“[The] most important legacy may be the dethroning of Jacobson…[which] has been the key precedent supporting vaccine mandates and other public health laws….With Jacobson apparently sidelined, the future of many public health laws, including and especially vaccine mandates, appears perilous.”
Background: “Up to 20% of people worldwide develop gastrointestinal symptoms following a meal, leading to decreased quality of life, substantial morbidity and high medical costs”
“Here we show that a bacterial infection and bacterial toxins can trigger an immune response that leads to the production of dietary-antigen-specific IgE antibodies in mice, which are limited to the intestine. Following subsequent oral ingestion of the respective dietary antigen, an IgE- and mast-cell-dependent mechanism induced increased visceral pain. This aberrant pain signaling resulted from histamine receptor H1-mediated sensitization of visceral afferents. Moreover, injection of food antigens (gluten, wheat, soy and milk) into the rectosigmoid mucosa of patients with irritable bowel syndrome induced local oedema and mast cell activation.”
My take: This study shows how innocuous food can trigger pain after an intestinal infection.