Link to full NASPGHAN 2019 Abstracts.
Here are some more abstracts/notes that I found interesting at this year’s NASPGHAN meeting.
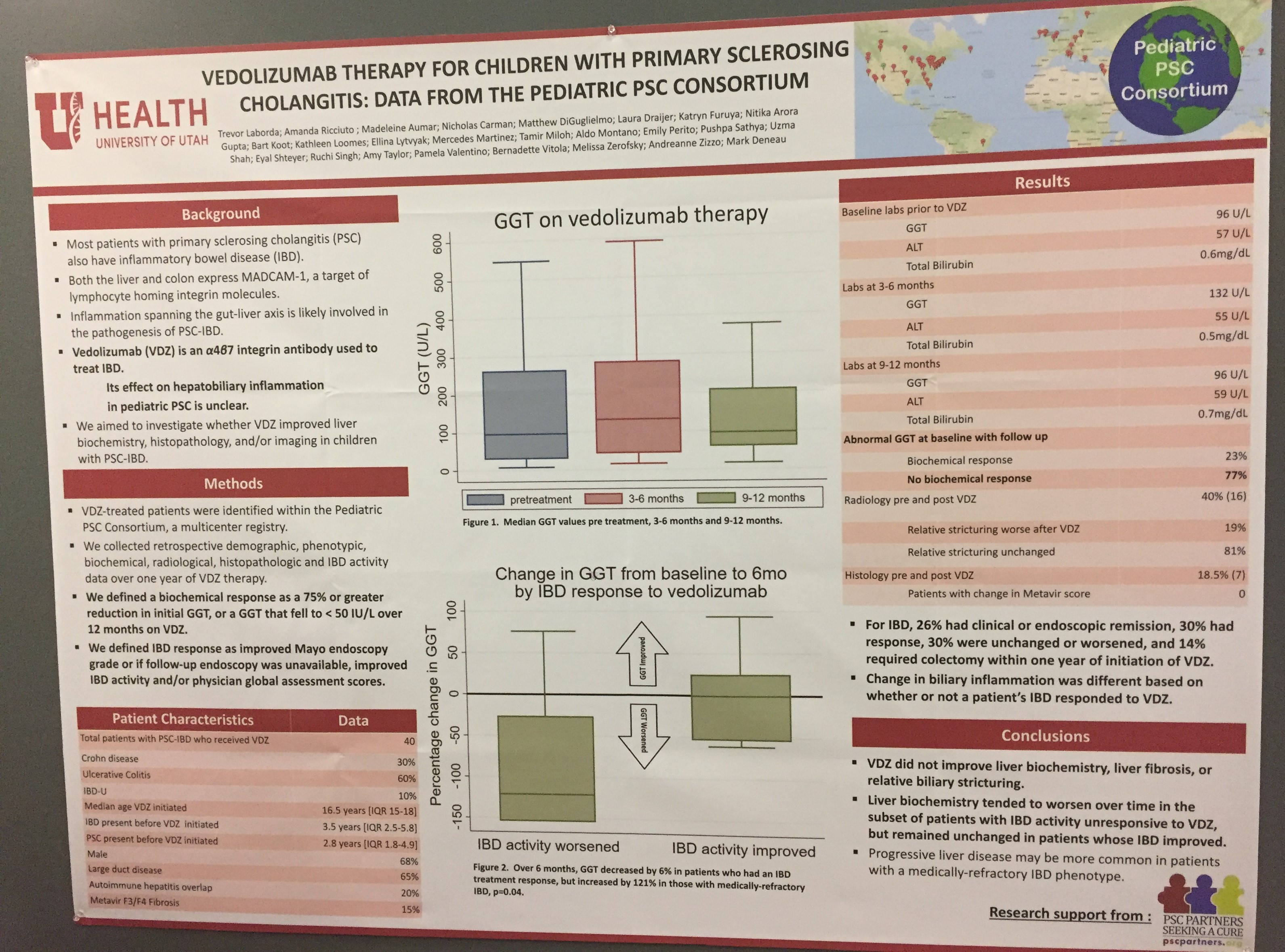
A study (poster below) from Cincinnati found that a vedolizumab level ≥34.8 mcg/mL at week 6 (prior to 3rd infusion) predicted clinical response at 6 months
Related blog posts:
- Getting the Most Out of Vedolizumab
- Proactive Therapeutic Drug Monitoring -Different Time Points
- Vedolizumab Drug Levels –Are They Needed?
- Therapeutic drug monitoring for vedolizumab
- A Bunch of Data on Vedolizumab

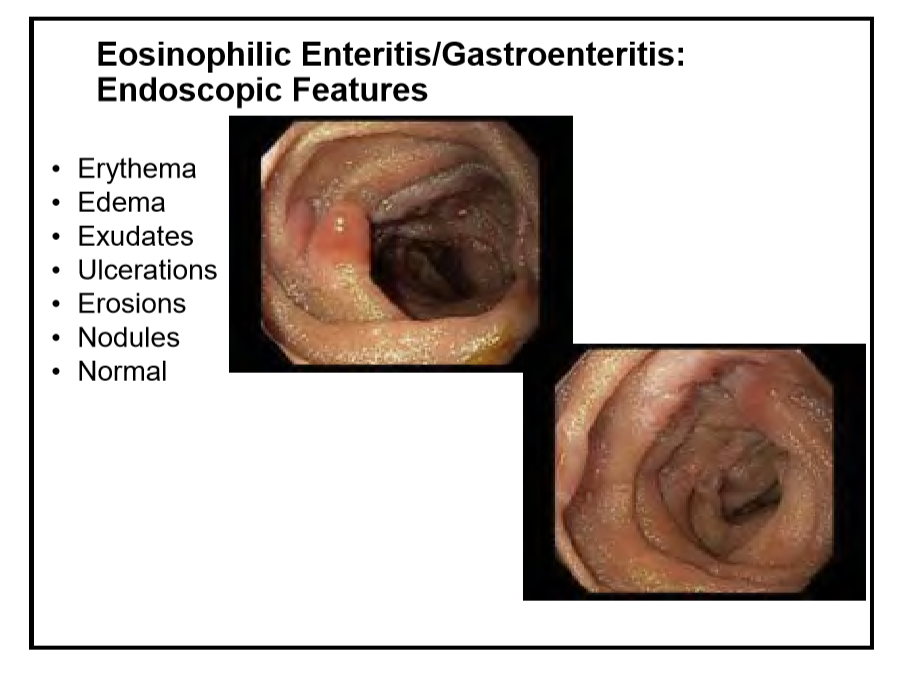
The poster below reported a high frequency of eosinophilic disorders in children who have undergone intestinal transplantation. Related blog post: Eosinophilic disease in children with intestinal failure

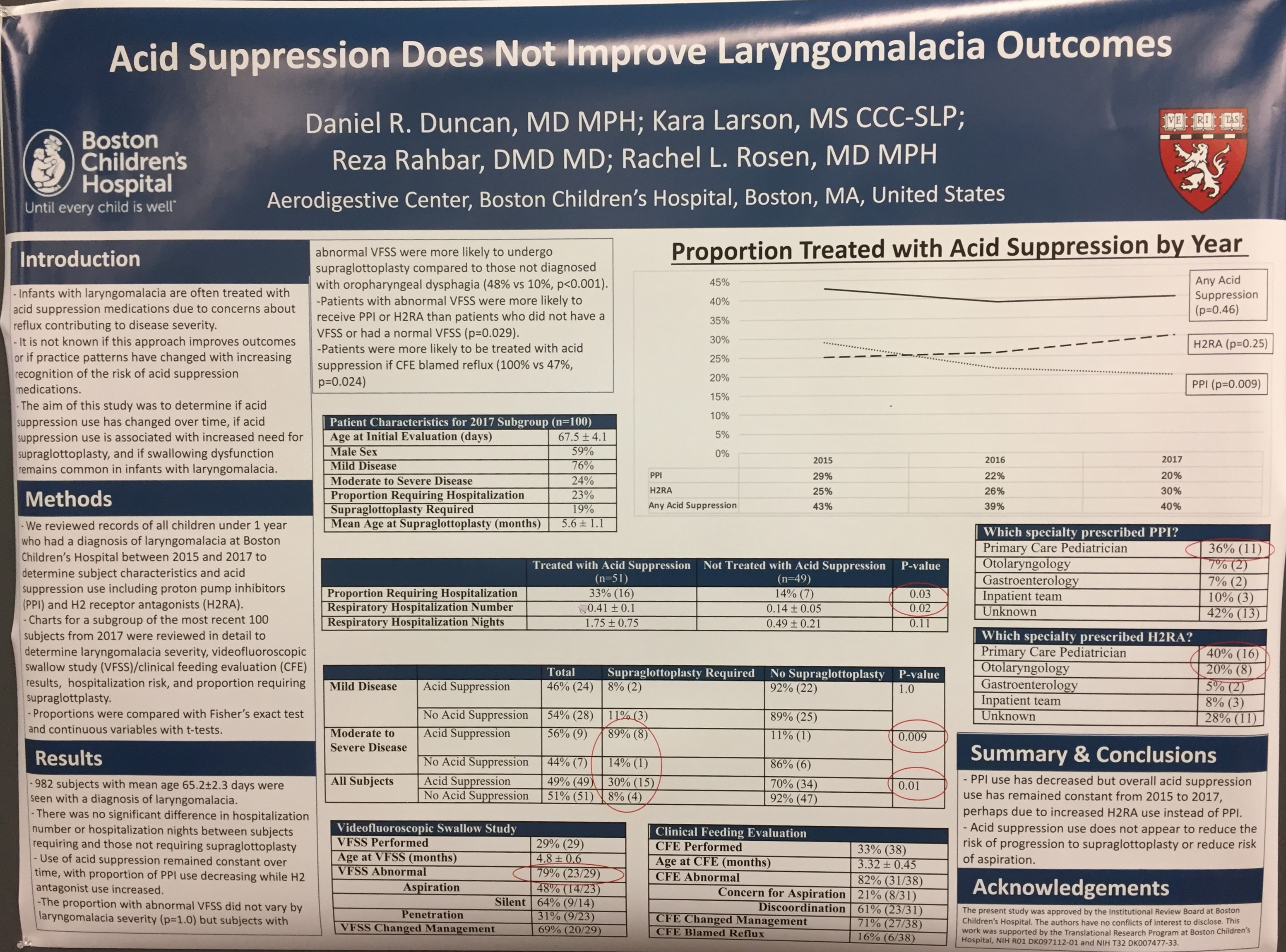
This study from Boston indicates that acid suppression was not associated with improved outcomes in infants with laryngomalacia (eg. lower supraglottoplasy rates or lower aspiration rates.
Related blog posts:
- Clinical evaluation not sensitive for aspiration
- Something Useful for Apparent Life-Threatening Events (ALTEs) [or BRUEs]
- What to do with ALTEs
- Does Reflux Lead to Increased Aspiration Pneumonia?
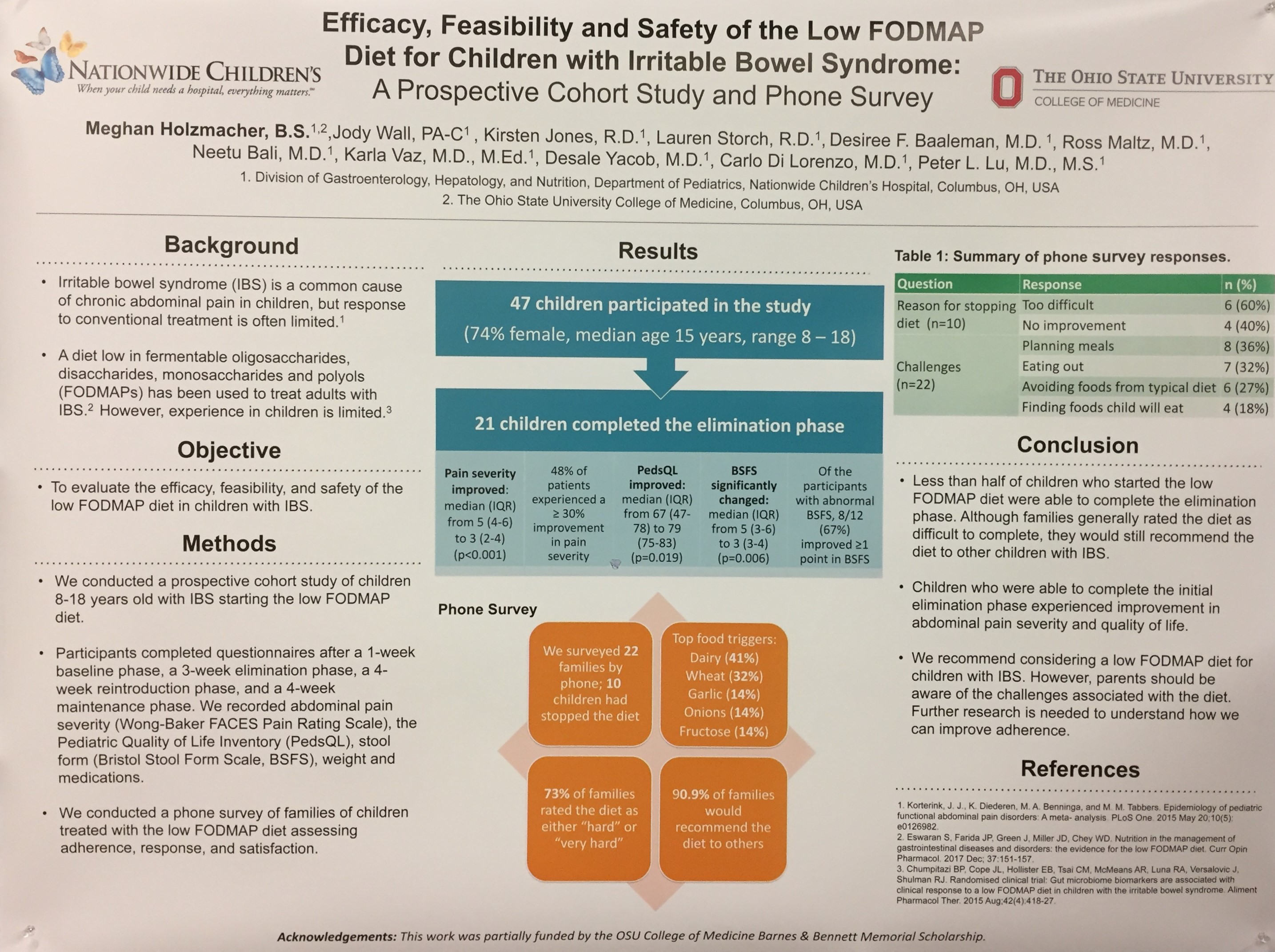
The study below showed that “less than half of children who started the low FODMAP diet were able to complete the elimination phase.” This indicates the need for careful dietary counseling when attempting this therapy.
Related blog posts:
- Newest FODMAPs Study for IBS | gutsandgrowth
- Mechanism for FODMAPs diet | gutsandgrowth
- Low-FODMAPs with or without Gluten-Free Diet in IBS | gutsandgrowth
- Low FODMAPs Diet in Pediatric Irritable Bowel | gutsandgrowth
- FODMAPS Advice From Harvard | gutsandgrowth
The abstract below showed that the dietary intake of children with inflammatory bowel disease, who were not receiving enteral nutrition therapy, was similar to healthy control children.


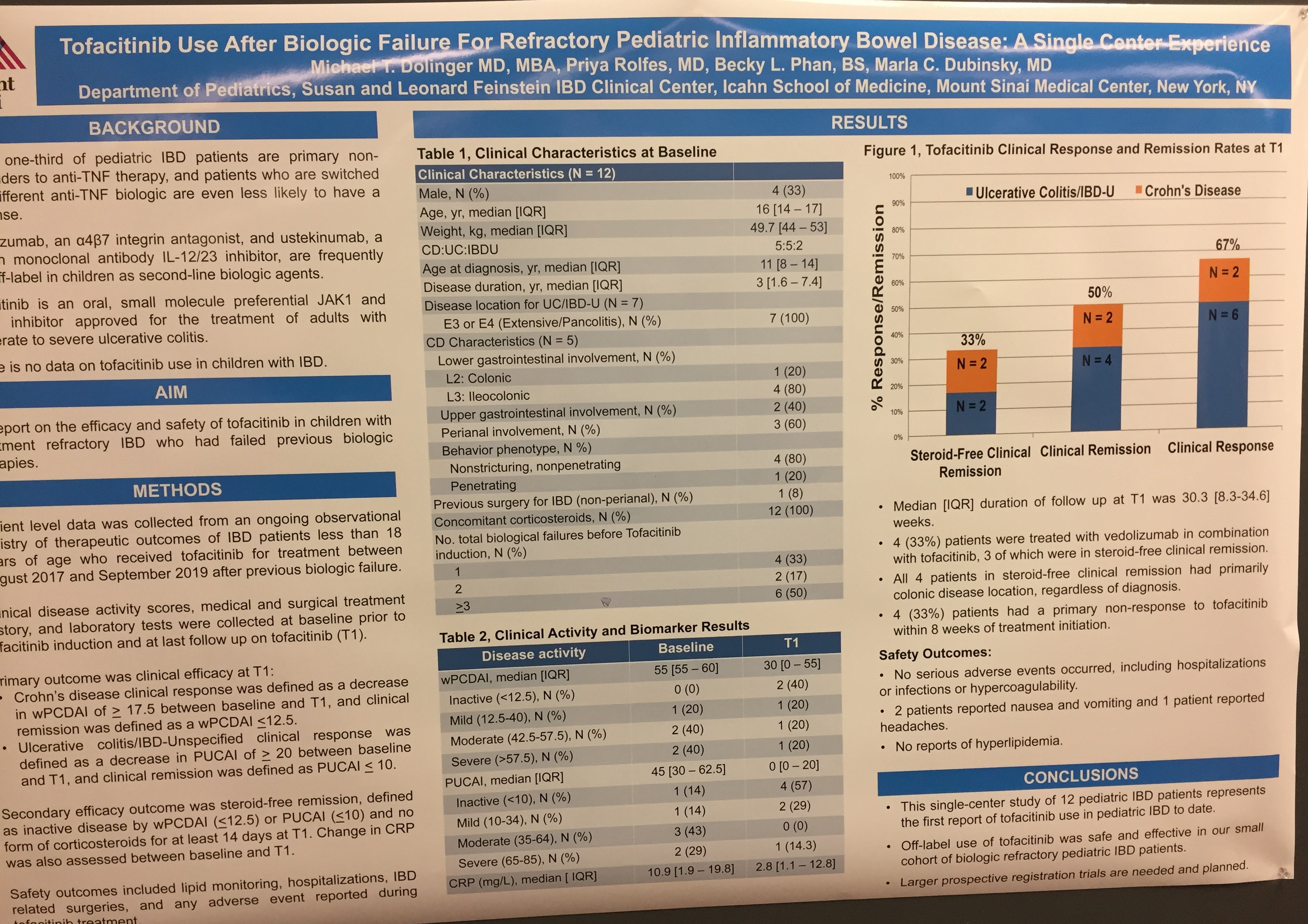
The next two studies provide some pediatric experience with tofacitinib in teenagers with inflammatory bowel disease (14-18 years of age). The first poster had 12 children and reported a 67% clinical response rate (cohort with 5 with CD, 5 with UC, and 2 with IC). The second poster had 4 of 6 with a clinical response and 3 in remission.
Related blog posts -Tofacitinib:
- Tofacitinib: a Jak of All Trades
- Tofacitinib: Where does it Fit in UC Treatment Algorithm?
- AGA Guidelines on the Management of Mild-to-Moderate Ulcerative Colitis
- Tofacitinib for Induction and Maintenance of Ulcerative Colitis
- Latest on Tofacitinib for Refractory Ulcerative Colitis
- Tofacitinib –a JAK Inhibitor for UC
- Tofacitinib -Risks and Benefits in Rheumatoid Arthritis

Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.