We had a terrific lecture given to our group by Rashelle Berry. She is a pediatric dietitian specializing in feeding disorders, enteral nutrition, and tube weaning. She practices within the Feeding Program at Children’s Healthcare of Atlanta, partnering closely with a wide variety of disciplines to care for children with significant feeding challenges and GI-related nutrition concerns. My notes below may contain errors in transcription and in omission.
Key Points:
- Families expectations are often at odds with dealing with tube feeding which makes it more difficult
- Parents have strong desire to achieve all oral feedings and often look for advice outside of clinical visits
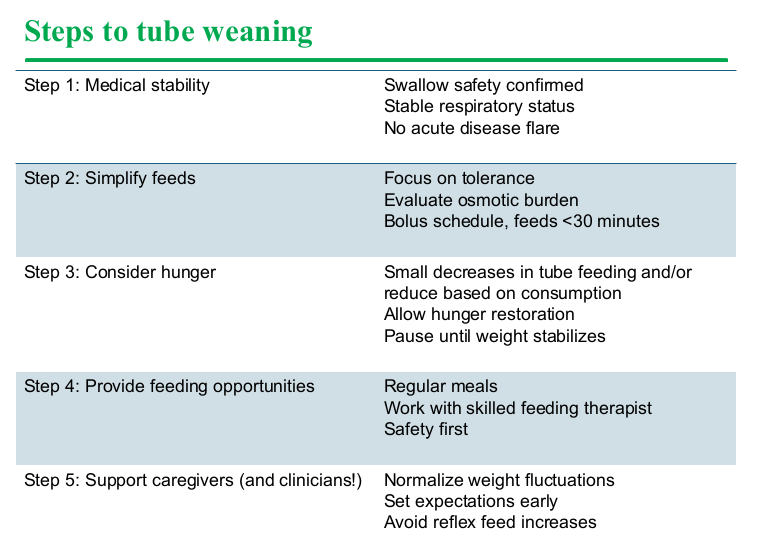
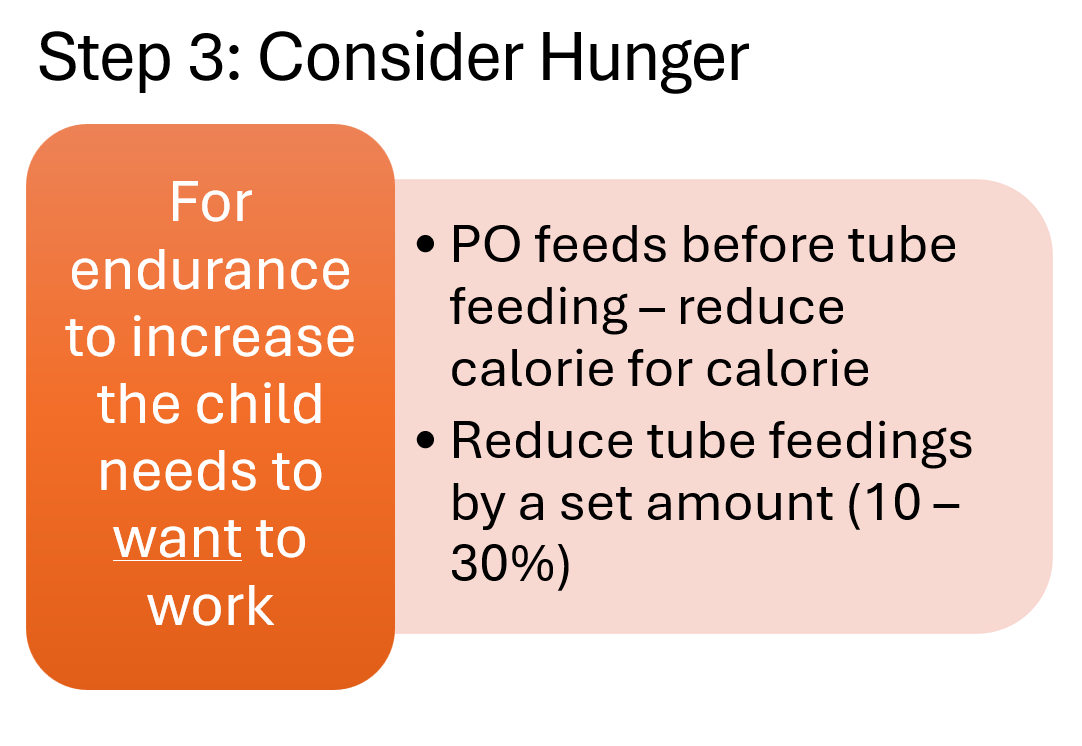
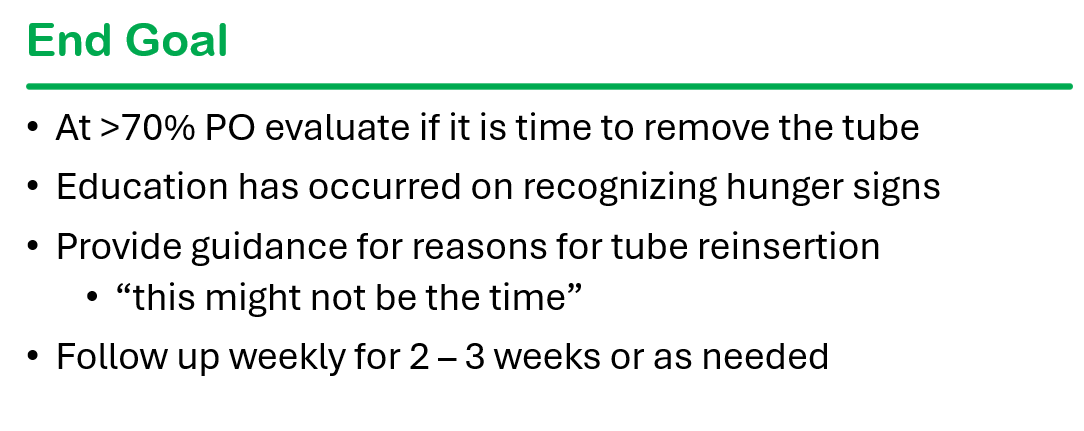
- Hunger alone is not sufficient to transition off tube feedings
- Prior to attempts to stop tube feedings, it is important to assess safety and to align feeding patterns to be more physiologic. This includes offering feeds via bolus typically every 3 hours and stopping continuous feedings
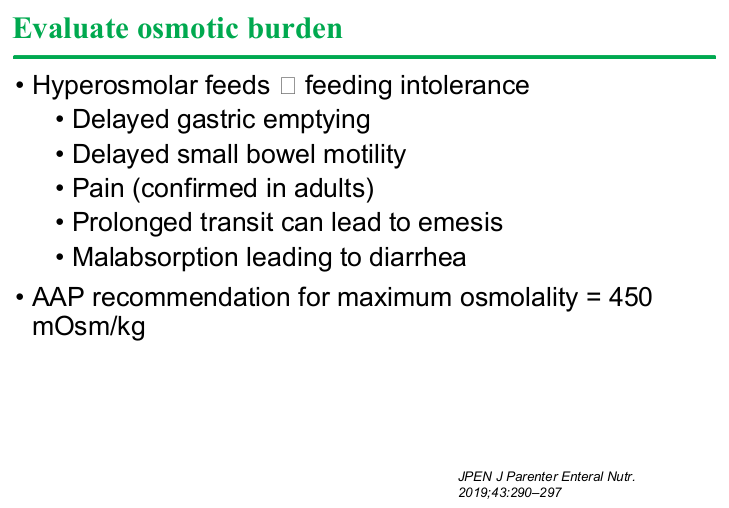
- Hyperosmolar feedings can contribute to GI symptoms
- Changing formula to improve tolerance can result in quick symptom improvement (1-2 days)
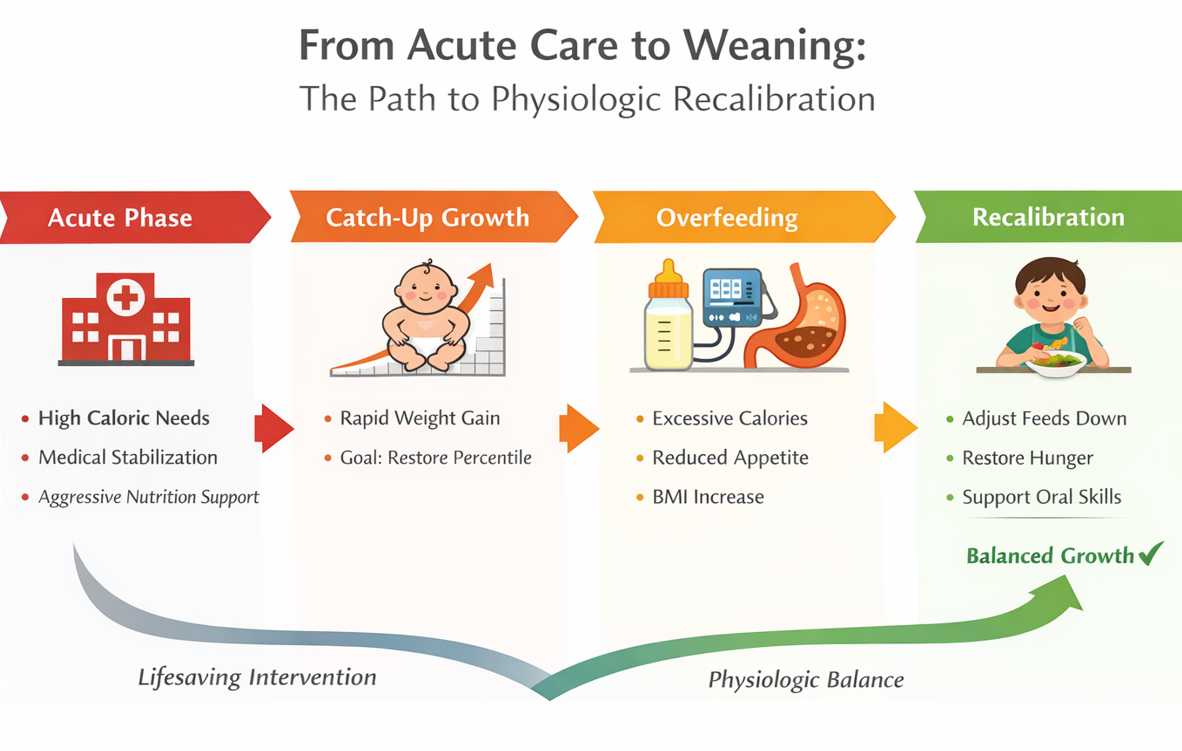
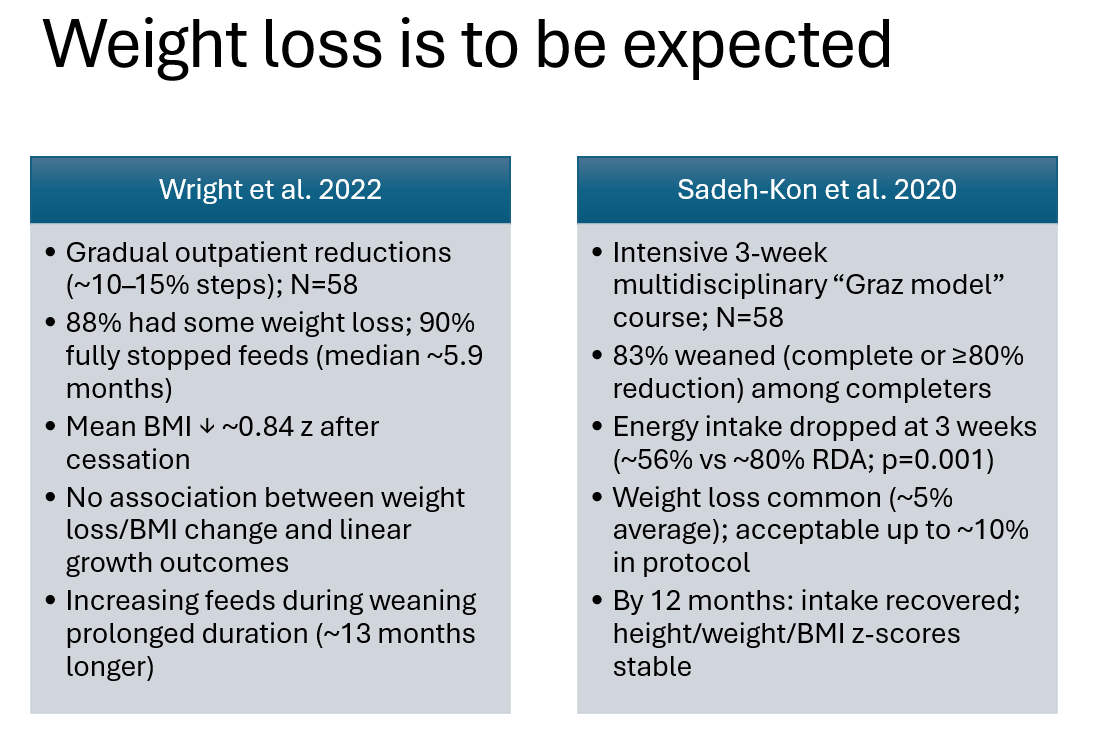
- Many children with tube feedings are overfed. This can contribute to poor hunger as well as initial weight loss when transitioning off tube feeds
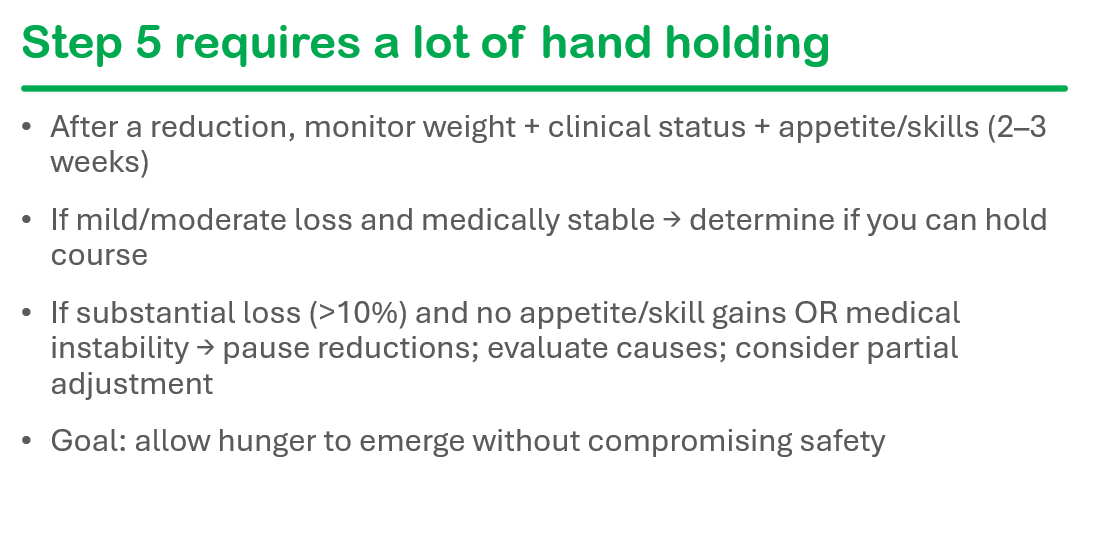
- Two main options to advance oral feedings: 1. Offer oral feeds prior to tube feeds and reduce tube feedings based on oral intake 2. Plan to reduce tube feedings by a set amount, typically 10-30% and follow to see if oral intake improves
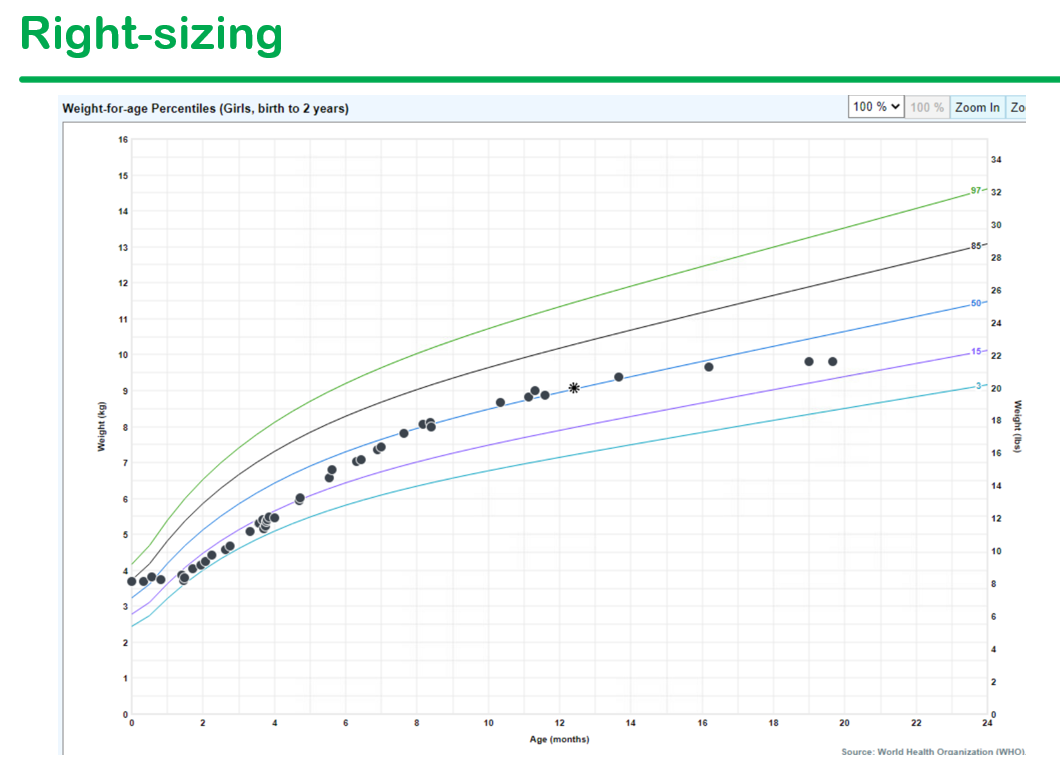
- Expect some weight loss during transition; if mild weight loss, most often continue to follow closely

Related blog posts:
- Dr. Praveen Goday: Tips on Managing Feeding Problems (Part 1)
- Dr. Praveen Goday: Tips on Managing Feeding Problems (Part 2)
- Durability of Intensive Feeding Therapy
- Data on Bridles -They Work!
- 5 Signs Your Child Needs a Feeding Tube
- Parent Perspective, Pediatric Nutritionist and Traci Nagy
- “Pediatric Formula Basics”
- NASPGHAN Toolbox App
- Websites recommended by GI families