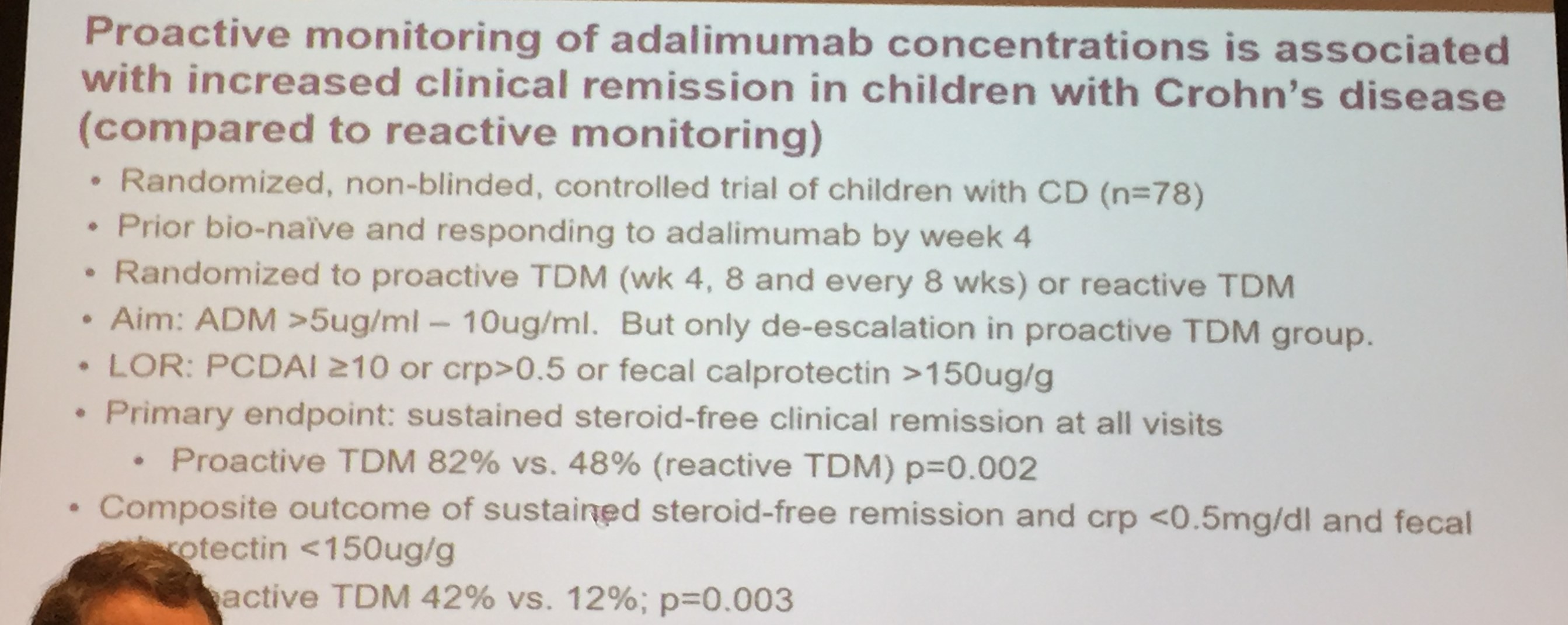
A nonblinded randomized controlled trial (A Assa et al. Gastroenterology 2019; 157: 985-06) with 78 children who had Crohn’s disease provides some of the best evidence to date that proactive therapeutic drug monitoring (pTDM) is important for anti-TNF therapy. The trial was called the PAILOT =Paediatric Crohn’s disease Adalimumab-Level-based Optimisation Treatment. This is the first RCT of pTDM that actually achieved its primary end point.
In this study, children were divided into a pTDM group (n=38) who received adalimumab levels at weeks 4 and 8 along with every 8 weeks unitl week 72. The control group (n=31) had reactive monitoring. The investigators aimed for a trough concentrations above 5 mcg/mL.
Key findings:
- The primary endpoint of sustained corticosteroid-free clinical remission (CFCR) was achieved in 82% of the pTDM group compared to 48% in the reactive monitoring group (p-.002).
- The pTMD also had a higher rate of the composite outcome (CFCR, CRP ≤0.5 mg/dL, and calprotectin ≤150): 42% compared to 12% in the control group (p=.003)
- 87% of pTDM had dose intensification compared to 60% in control group.
The editorial by Papamichael and Cheifetz (pg 922-4) highlights some additional observations:
- “The study actually showed that a 10.0 mcg/mL threshold performed better than 7.5 and 5.0 mcg/mL” with respect to PCDAI and CRP levels.
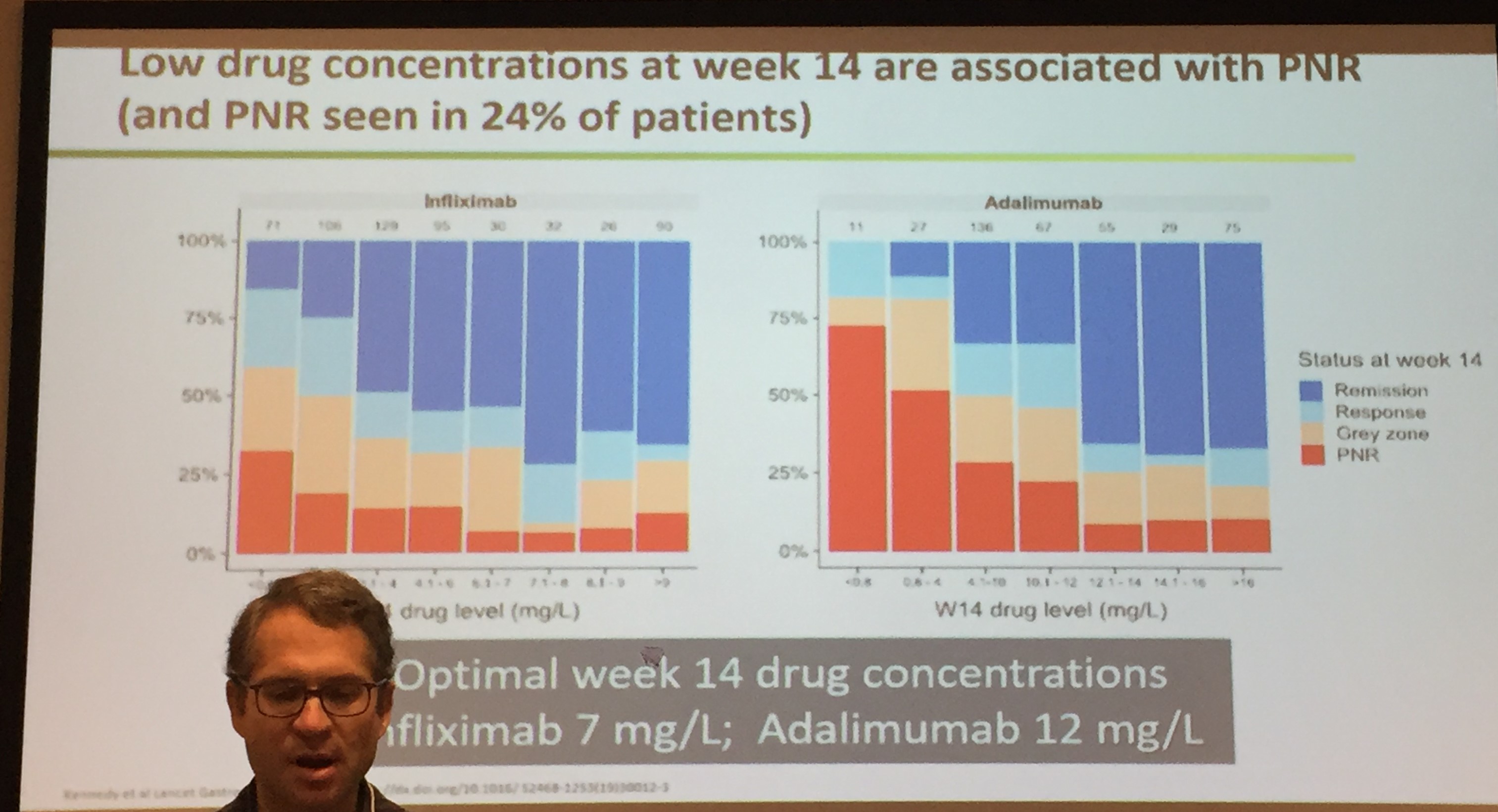
- “The recent prospective Personalized anti-TNF therapy in Crohn’s disease study (PANTS) showed that the optimal week 14 adalimumab concentration …at both week 14 and 54 was 12 mcg/mL”
My take: Most pediatric gastroenterologist understand the importance of pTDM, especially as conventional dosing of anti-TNF agents is often too low. This study provides some needed proof and hopefully will aid our efforts to get adequate insurance coverage. The optimal frequency and timing of pTDM still needs work.
Related blog posts:
- CCFA 2019 Update: Proactive Therapeutic Drug Monitoring
- Appropriate Proactive Therapeutic Drug Monitoring
- Briefly noted: Induction Infliximab Levels
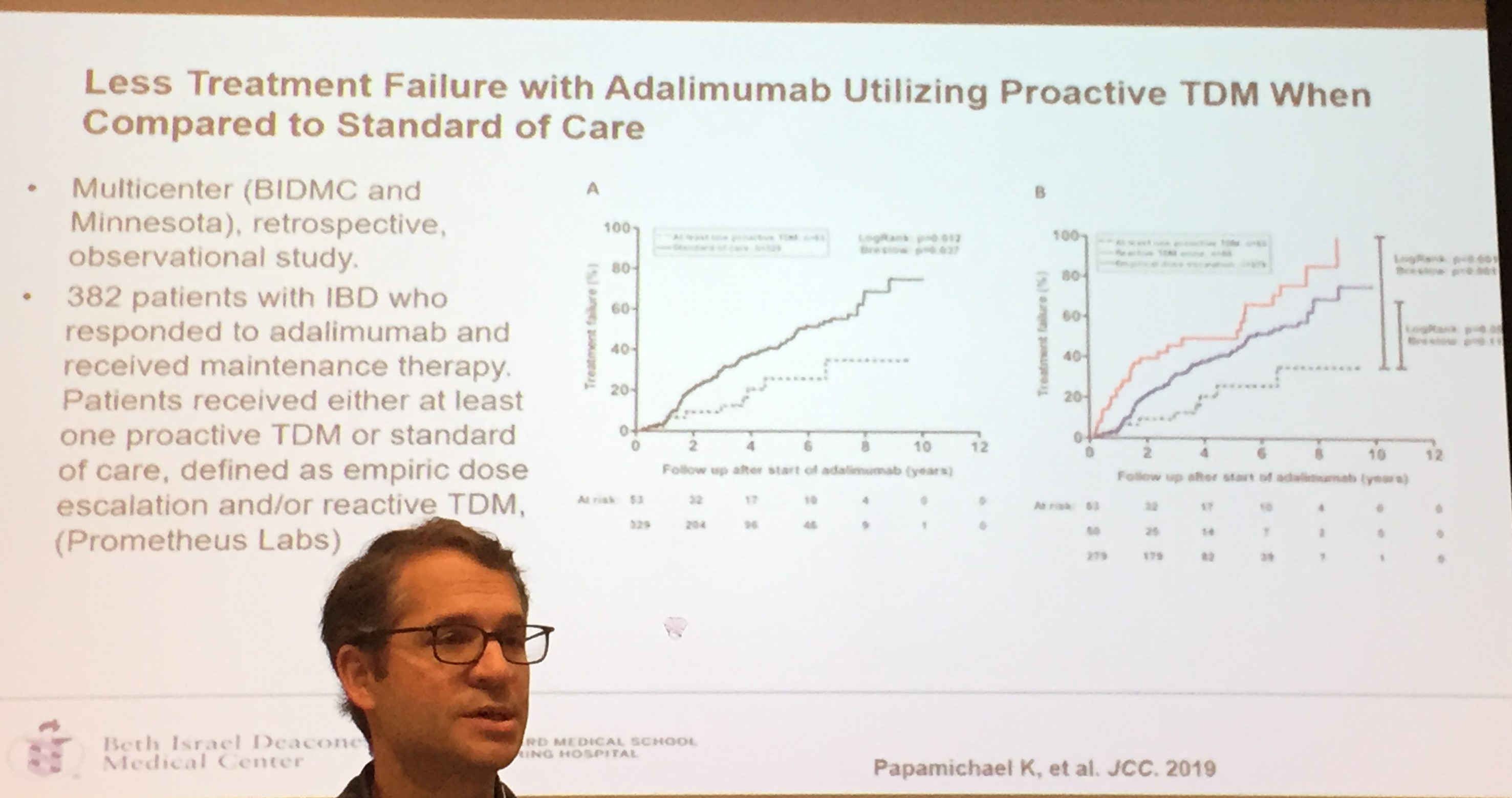
- Is there good evidence for proactive therapeutic drug monitoring of anti-TNF therapy?
- Is Standard Infliximab Dose Too Low in Pediatrics?
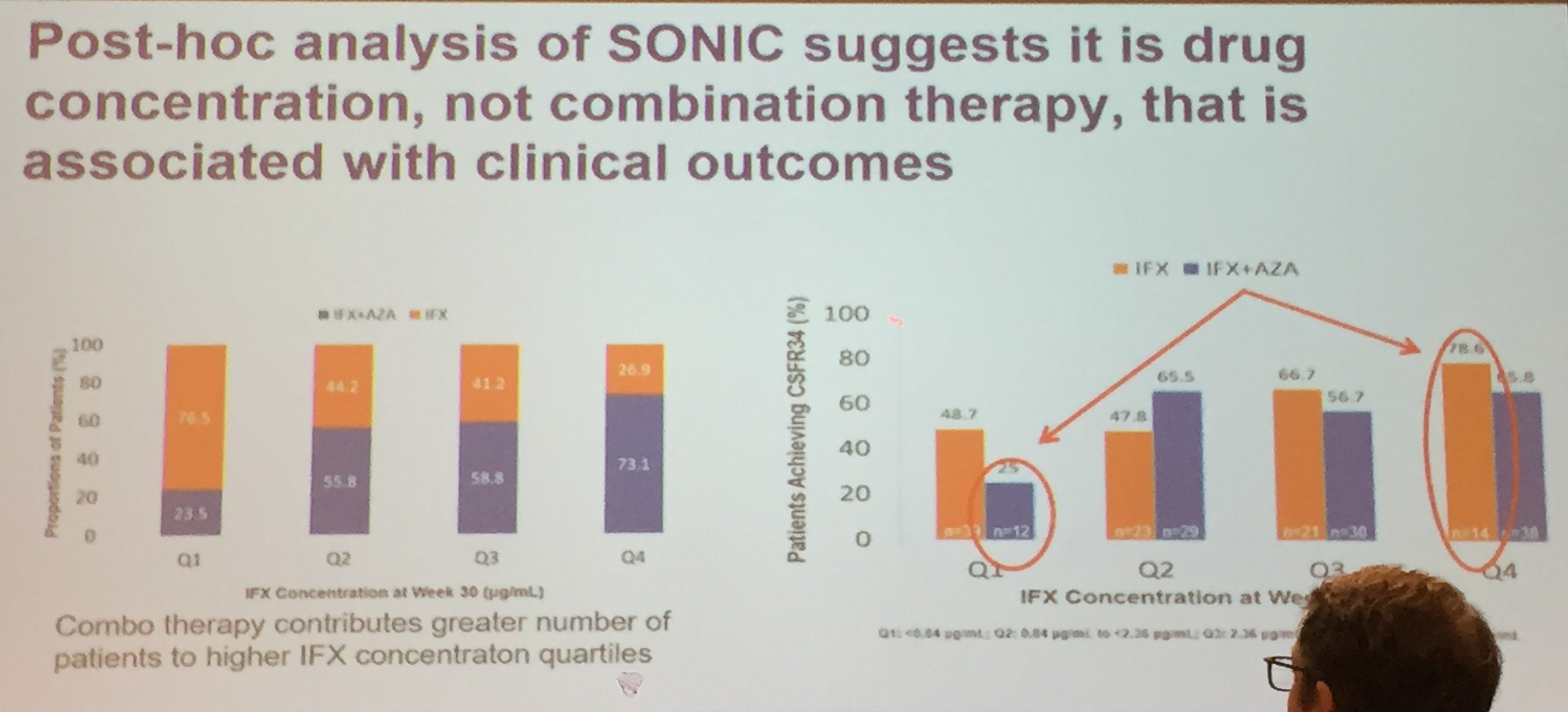
- Can Therapeutic Drug Monitoring with Monotherapy Achieve Similar Results as Combination Therapy for IBD? | gutsandgrowth
- AGA 2017 Guidelines on Therapeutic Monitoriing Proactive drug monitoring: “careful and selective use of proactive TDM could be beneficial, but current evidence for its routine use is limited and its overall benefits remain uncertain”
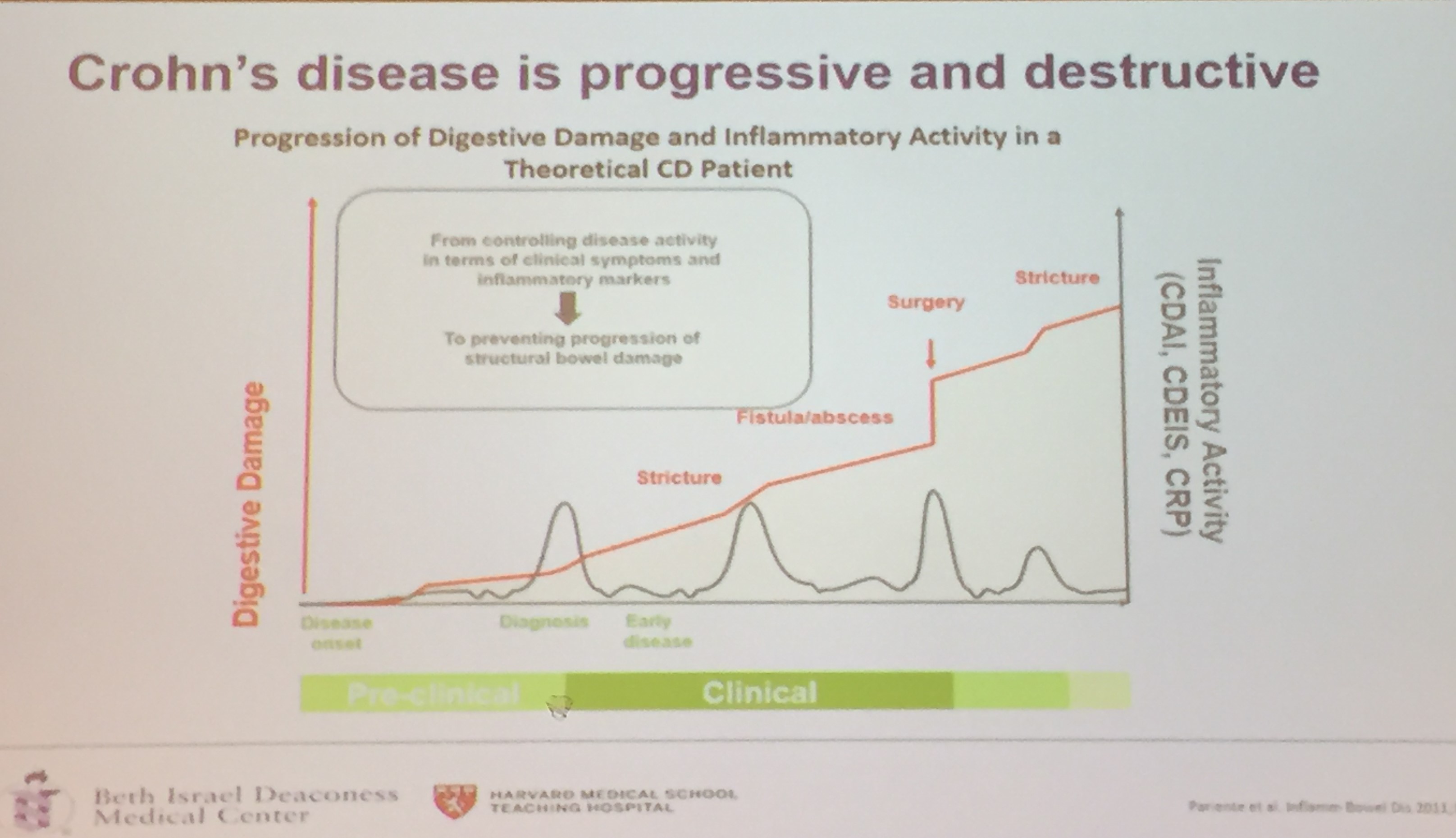
- “Silent” Crohn’s Disease | gutsandgrowth
- Treating to Target | gutsandgrowth
- New Target Drug Levels in Inflammatory Bowel Disease | gutsandgrowth

I really enjoyed my recent trip to Chicago. Here’s a picture from Lincoln Park Zoo from my favorite photographer