One useful resource for NASPGHAN members (NASPGHAN Nutrition Pearls) has been the short monthly nutrition pearl videos (about 10 of them so far). Here are some pointers from the most recent of these.
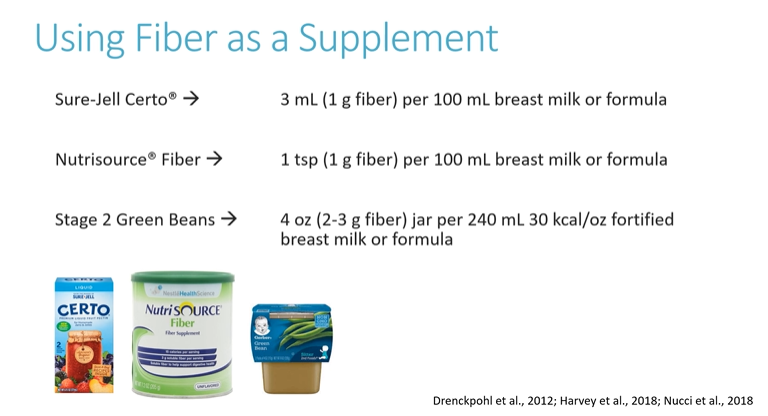
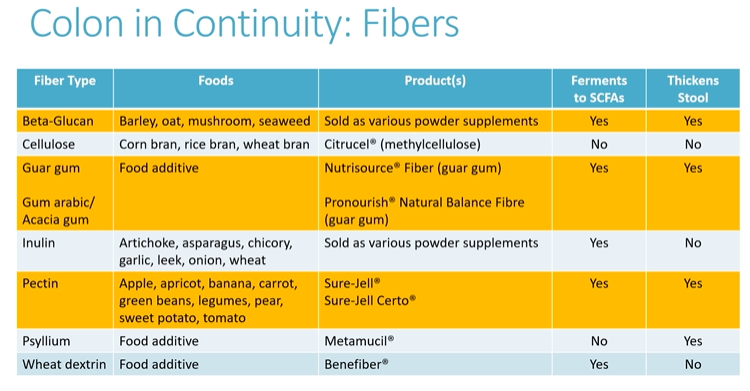
In October: Fiber for Short Bowel Syndrome –Beneficial for those with a colon in continuity:
In September: Growth in Cystic Fibrosis


Related blog posts for Short Bowel Syndrome:
- Short Gut Diet -CHOA Approach
- #NASPGHAN19 Intestinal Failure Session (Part 2)
- N2U -Part 2: Poor Growth and Short Bowel Syndrome | gutsandgrowth
- Green Beans for Short Gut Syndrome
- Enteral Autonomy in Pediatric Intestinal Failure | gutsandgrowth
- Medical Progress for Intestinal Failure Associated Liver Disease | gutsandgrowth
- Nutrition Support for Intestinal Failure | gutsandgrowth
- Using Spot Urine Sodiums | gutsandgrowth
- Predicting Short Bowel Syndrome Enteral Autonomy: Small Bowel Diameter | gutsandgrowth
Related blog posts for Cystic Fibrosis:
- Big Advance for Cystic Fibrosis -Who Will Benefit?
- Complex Family of CFTR-Associated Disorders
- Lumacaftor-Ivacaftor for Cystic Fibrosis
- Ivacaftor for Cystic Fibrosis | gutsandgrowth
- CFTR Modulators for Cystic Fibrosis
- FDA Expands Use of Cystic Fibrosis Medication | gutsandgrowth
- “Origins of Cystic Fibrosis Lung Disease”
- Stratifying Cystic Fibrosis Liver Disease with Ultrasonography | gutsandgrowth