7/1/24 FDA approves biosimilar Pyzchiva® (ustekinumab-ttwe), to be commercialized by Sandoz in US

N Sengupta et al. Am J Gastroenterol 2024; 119: 438-449. Open Access! The Role of Imaging for Gastrointestinal Bleeding: Consensus Recommendations From the American College of Gastroenterology and Society of Abdominal Radiology. Thanks to Dr. Benjamin Gold for this reference.
This article was jointly published: Radiology 2024; 310(3):e232298
This article focuses on GI bleeding in adults; it has a lot of useful information about the advantages, disadvantages, techniques and performance date of numerous radiology tests which can help sort out GI bleeding.
Some of the recommendations for Overt Lower GI Bleeding:
CT Angiography:

Catheter Angiography:

99mTc-RBC Scan

For Suspected Small Bowel Bleeding:
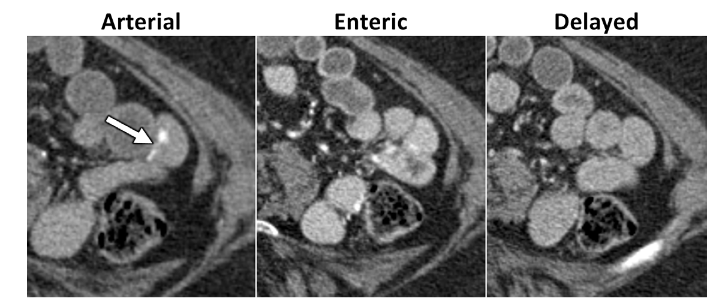
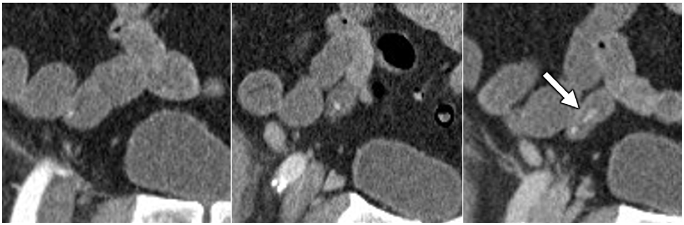
CT Enterography (uses oral contrast). Technique: CTE should be performed using multiphase technique in patients older than 40 years of age where vascular lesions are a common cause for bleeding.

Meckel’s Scan “A Meckel scan can be considered to identify the cause of unexplained intermittent GI bleeding in children and adolescents after negative endoscopic evaluation, including capsule endoscopy if available, and cross-sectional evaluation of the small bowel.”
Radiology compared to capsule endoscopy and balloon-assisted endoscopy The authors discuss the advantages and limitations of radiologic testing versus capsule endoscopy and balloon-assisted endoscopy for small bowel bleeding is provided in Appendix S5
My take: This article provides a good update/review on useful radiologic imaging for GI bleeding. For pediatric GI bleeding, the etiologies are much different and many patients should be evaluated with a Meckel’s scan prior to panendoscopy (depending on the clinical presentation).
Related blog posts:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
BE Hansen et al. Hepatology 2024; 79: 1279-1292. Open Access! Event-free survival of maralixibat-treated patients with Alagille syndrome compared to a real-world cohort from GALA
This study compared “6-year outcomes from maralixibat trials with an aligned and harmonized natural history cohort from the Global ALagille Alliance (GALA) study.”
Based on a quick review, some the data appears to overlap a recent report in the same journal: RJ Sokol et al. Hepatology 2023; 78: 1698-1710. Open Access! Predictors of 6-year event-free survival in Alagille syndrome patients treated with maralixibat, an ileal bile acid transporter inhibitor (See blog post: Six Year Data for IBAT Inhibitor Treatment for Alagille Syndrome).
In the current study, “event-free survival, defined as the time to first event of manifestations of portal hypertension (variceal bleeding, ascites requiring therapy), surgical biliary diversion, liver transplant, or death, was analyzed by Cox proportional hazards methods.”
Key findings:
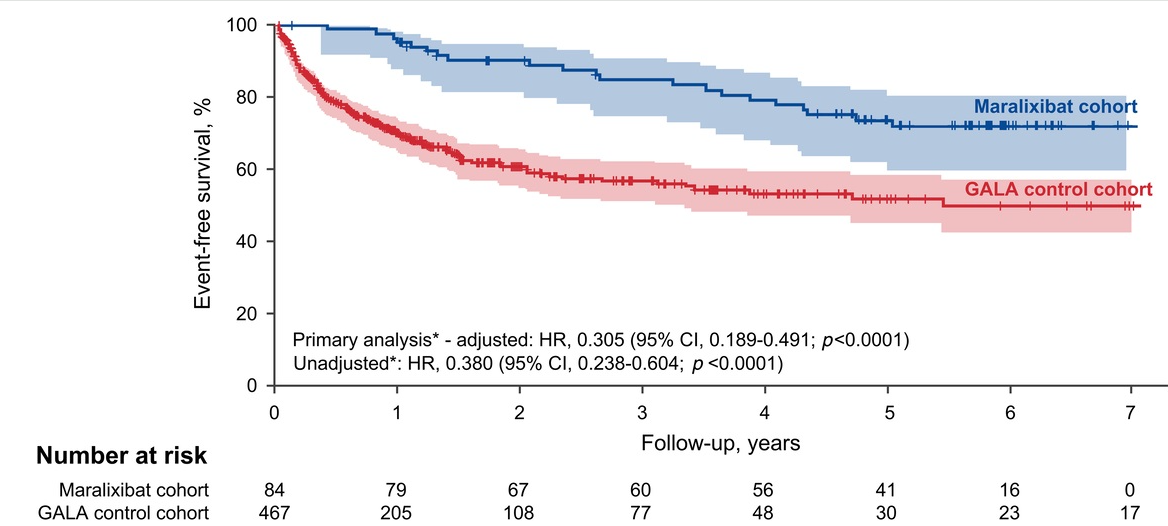
In their discussion, the authors note that much of the improvement in event-free survival is due to improvement in pruritus which is a main indication for liver transplantation. They speculate that improvement in event-free survival is also related to more broad-based clinical improvement (observed in ICONIC study), perhaps due to reduction in retained hepatic bile acids.
One of the limitations, reliance on a historical control, is discussed. “Historical control comparison is useful when there are ethical concerns regarding the recruitment of patients for long-term control arms requiring several years of study in life-threatening or debilitating diseases.”
My take: In this real-world comparison, Maralixibat, clearly was associated with improved outcomes. How much of this was due to relief of intractable pruritus and how much of this may be due to other biologic factors remains uncertain.
Related blog posts:
R Michael, J Tozer. N Engl J Med 2024;390: e53. Small-Bowel Intussusception in an Adult
The authors describe the presentation/resolution of a 57 yo with a small bowel intussusception due to a fibroblastic polyp lead point.
Video: Reduction of Intussusception (may be behind a paywall)


Related blog posts:
M Chehade et al. NEJM 2024;390:2239-2251 Dupilumab for Eosinophilic Esophagitis in Patients 1 to 11 Years of Age
This study provides published data that has been referenced previously at time of FDA approval and prior meetings (see posts: Dupixent Approved in Younger Children (15 kg+), Dupixent for Eosinophilic Esophagitis (1-11 yrs) and Clinical Diagnosis of Rumination from DDW Tweets).
Methods:
Key findings:
My take: Dupilumab is an effective option for eosinophilic esophagitis.
Related blog posts:




TC Tang et al. JPGN 2024;78:1317–1328. Proton pump inhibitors, antibiotics, and atopy increase the risk of eosinophilic esophagitis in children with esophageal atresia
In this retrospective study (2005-2020) with 184 children, key findings:
Discussion: “This is congruent with the emerging evidence in the general pediatric population that there is an increased risk of EoE development in individuals who undergo acid suppressive therapy. A possible explanation for these findings is that acid suppressants inhibit gastric parietal cell function and elevate the gastric pH, thereby impairing peptic digestion of dietary allergens, potentiating sensitization, and facilitating the development of allergic diseases like EoE.” Other potential explanations could include PPIs could increase mucosal permeability and/or contribute to dysbiosis.
“Hence, the routine use of PPIs for the first year of life as recommended by the current guidelines may need to be revisited..”
My take: This study shows a clear association of PPIs with development of EoE in this cohort. Due to the study design, it is difficult to be confident regarding causality due to possible selection bias (patients who received PPIs may be those with more predisposition to EoE). Nevertheless, this study suggests that prolonged use of PPIs, even in groups at risk for reflux damage, needs to be carefully considered and possibly directed by objective markers of reflux.
Related blog posts:

H Szajewska et al. JPGN 2024; https://doi.org/10.1002/jpn3.12280. Open Access! Early diet and the risk of coeliac disease. An update 2024 position paper by the ESPGHAN special interest group on coeliac disease
Key points:

Related blog posts:
AJ Sanyal et al. NEJM 2024; DOI: 10.1056/NEJMoa2401755. A Phase 2 Randomized Trial of Survodutide in MASH and Fibrosis
Background/Methods: “Dual agonism of glucagon receptor and glucagon-like peptide-1 (GLP-1) receptor may be more effective than GLP-1 receptor agonism alone for treating metabolic dysfunction–associated steatohepatitis (MASH). The efficacy and safety of survodutide (a dual agonist of glucagon receptor and GLP-1 receptor) in persons with MASH and liver fibrosis” was studied in “48-week, phase 2 trial, we randomly assigned adults with biopsy-confirmed MASH.” (n=293)
“Dual agonism of glucagon receptor and GLP-1 receptor may be more effective than GLP-1 receptor monoagonism for treating MASH, because the extrahepatic benefits of GLP-1 receptor agonism (glucose control, reduced appetite, and weight loss) are combined with direct hepatic effects (increased energy expenditure, lipolysis, and mobilization of hepatic fat) associated with glucagon receptor agonism.”
Key findings:
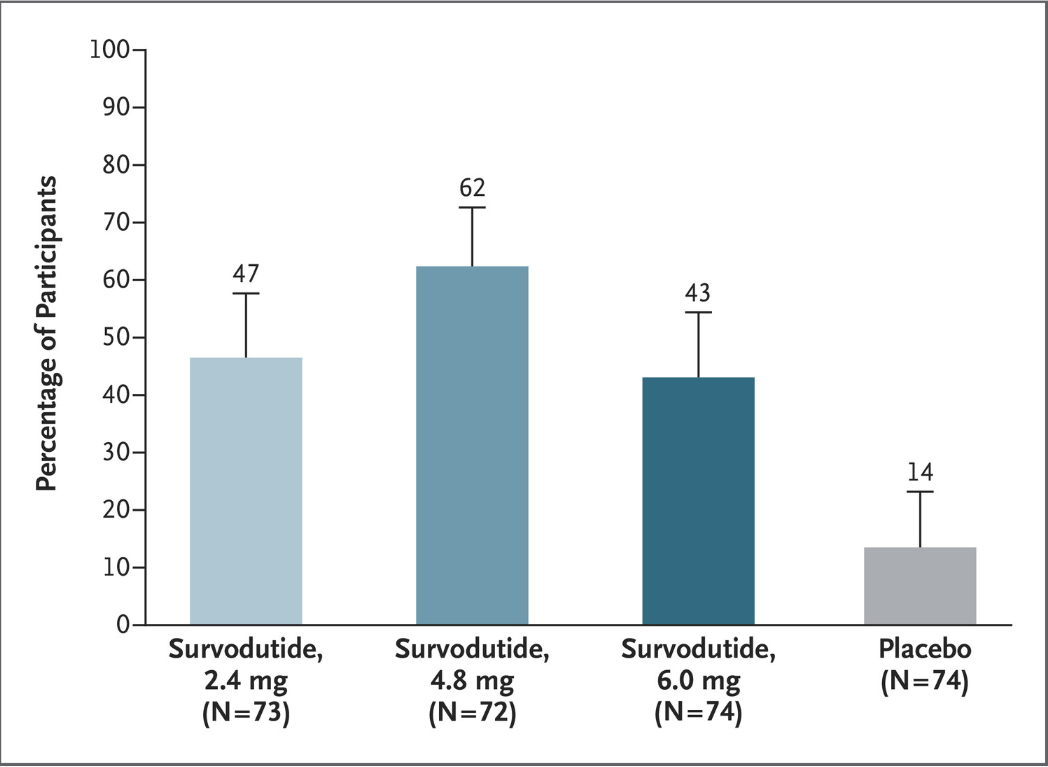
The discussion notes that “in a phase 2 trial, treatment with the GLP-1 receptor monoagonist semaglutide resulted in a significantly higher percentage of patients with MASH resolution than placebo but not in a significantly higher percentage of patients with improvement in fibrosis stage.26” Thus, the improvement in fibrosis, which was seen in this study with survodutide,will need to be examined in future studies.
My take: Earlier this year, the selective thyroid hormone receptor beta agonist resmetirom gained conditional approval from the Food and Drug Administration as the first pharmacotherapy for MASH with moderate-to-advanced liver fibrosis.5 It looks like there will be a number of pharmacologic agents available in the coming years. Cost and availability will be ongoing concerns. In addition, determining when/how these agents will be used in the pediatric population will not be clear for quite a long time.
Related blog posts:
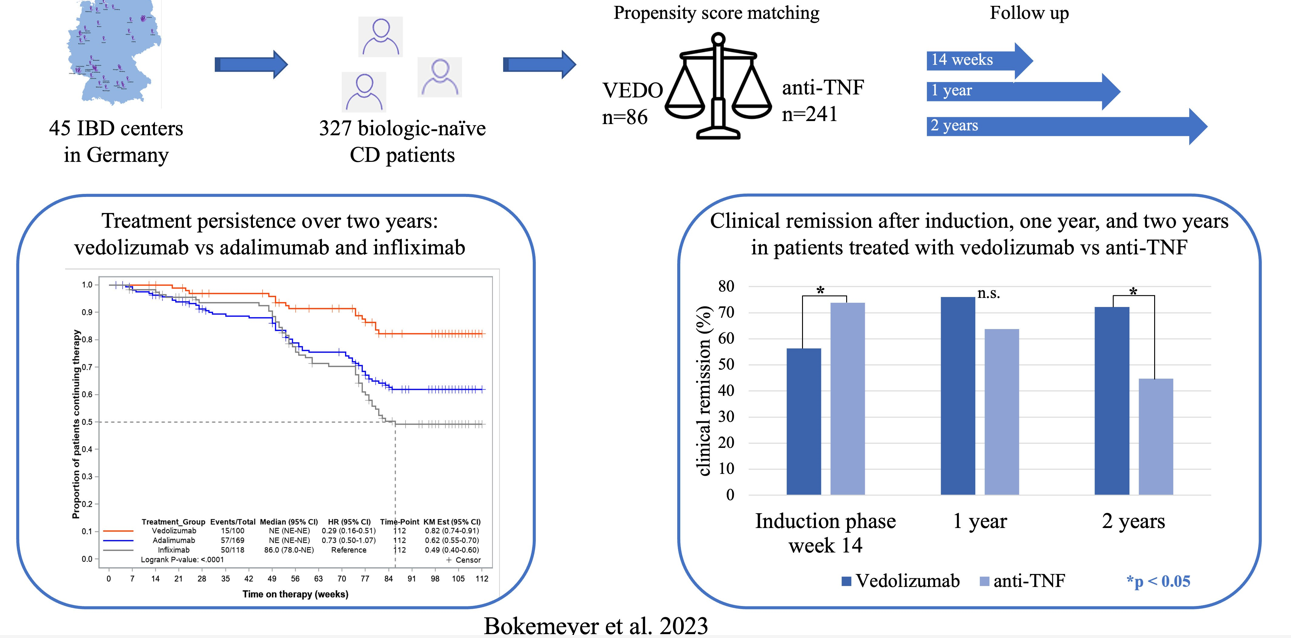
B Bokemeyer et al. Inflamm Bowel Dis 2024; 30: 746-756.
Methods: 3277 adult biologically-unexposed CD patients starting therapy with VEDO or anti-TNF were consecutively enrolled in 45 IBD centers across Germany (2017-202). This was a non-randomized, observational study with prospectively collected data.
Findings:
The discussion describes the strengths and limitations of this study. As it is not a randomized control trial, there can still be selection bias and confounding even with propensity scoring that was done in this study. The authors note that in a prior analysis of RCTs comparing infliximab to vedolizumab in CD patients, that infliximab had higher efficacy for induction and maintenance, though the clinical remission rates were only modestly improved at 1 year. (L Peyrin-Biroulet et al. BMC Gastroenterol 2022; 22: 291).
Recent expert guidance (2024) has favored infliximab and risankizumab over other advance therapies in CD patients who have not had previous biologic therapies (see: Comparative Evidence and Positioning Advance Therapies for Inflammatory Bowel Disease).
My take: This study shows that vedolizumab is a good advanced therapy for patients with Crohn’s disease without prior therapy. Among those with a clinical response at 14 weeks, the treatment durability was particularly impressive in this cohort.
It would be great to see an RCT in children with CD comparing IFX to VEDO. Treatment persistence is even more important in younger patients.
Related blog posts:
NBC News 5/14/24: Wegovy users keep weight off for 4 years, new analysis finds
“The 17,604-patient trial tested Wegovy not for weight loss but for its heart protective benefits for overweight and obese patients who had preexisting heart disease but not diabetes. Participants were not required to track diet and exercise because it was not an obesity study…”
“Patients in the trial, called Select, lost an average of nearly 10% of their total body weight after 65 weeks on Wegovy. That percentage weight-loss was roughly sustained year-on-year until the end of about four years, where weight loss stood at 10.2%…”
“A third new analysis on Select published by Novo on Tuesday showed that the heart protective benefits of Wegovy to patients in the trial occurred regardless of their weight before starting on the drug and regardless of how much weight they lose on it.”
“The weight loss in the heart trial was less than the average of 15% weight loss in earlier Wegovy obesity studies”
Related blog posts:

