S Wharton et al. NEJM 2023; DOI: 10.1056/NEJMoa2302392. Daily Oral GLP-1 Receptor Agonist Orforglipron for Adults with Obesity
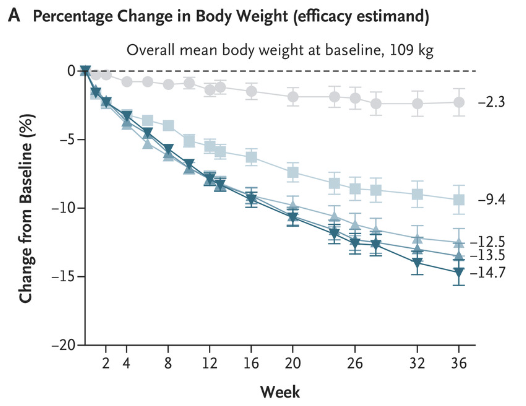
In this phase 2 randomized, double-blind trial with 272 adults with obesity (mean weight at baseline 108 kg), participants were randomly assigned to receive orforglipron at one of four doses (12, 24, 36, or 45 mg) or placebo once daily for 36 weeks. “The pharmacokinetic profile of orforglipron, with a half-life of 29 to 49 hours, supports once-daily oral administration.”
Key findings:
At week 36, the mean change ranged from −9.4% to −14.7% with orforglipron and was −2.3% with placebo.
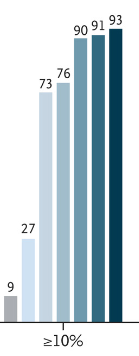
A weight reduction of at least 10% by week 36 occurred in 46 to 75% of the participants who received orforglipron, as compared with 9% who received placebo.
Adverse events reported with orforglipron were similar to those with injectable GLP-1 receptor agonists.
Weight reduction of at least 10% at week 36:
My take: This is an exciting time for drug development for obesity. Given the low success rates of traditional ‘lifestyle’ management approaches, these medications have the potential to reduce a great deal of morbidity. Oral agents, rather than injections, would hasten the use of these agents more broadly. Long term outcomes are still unclear.
AM Jastreboff et al. NEJM 2023; DOI: 10.1056/NEJMoa2301972. Triple–Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial.
Background: Retatrutide (LY3437943) is an agonist of the glucose-dependent insulinotropic polypeptide, glucagon-like peptide 1, and glucagon receptors.
Methods: This study enrolled 338 with BMI of at least 27 in a a phase 2, double-blind, randomized, placebo-controlled trial with once-weekly injections of retatrutide.
Key Findings:
The number who achieved at least a 10% weight loss:
“The safety profile of retatrutide was consistent with reported phase 1 findings in persons with type 2 diabetes13 and similar to those of therapies based on GLP-1 or GIP–GLP-1 for the treatment of type 2 diabetes or obesity”
My take: There are a number of effective agents for obesity that have been developed very recently. Long term efficacy and safety are still not well-understood.
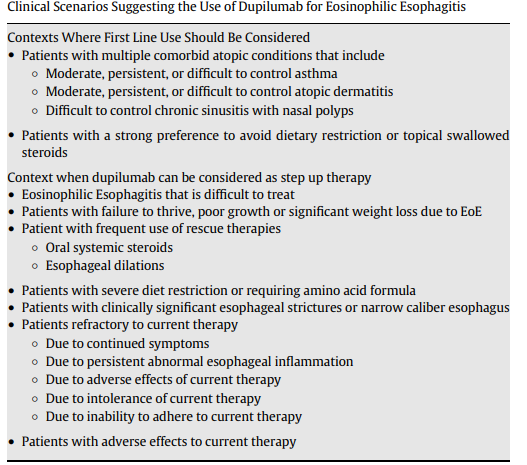
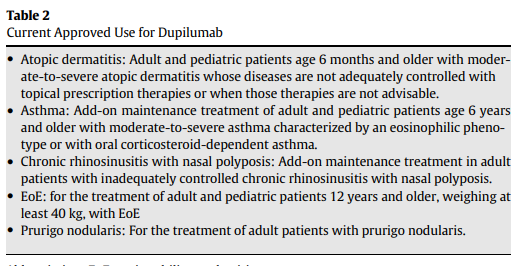
This article summarizes updated recommendations for eosinophilic esophagitis from the Joint Task Force for the American Academy of Allergy Asthma Immunology and American College of Allergy Asthma Immunology and the American Gastroenterology Association (JTF-AGA). It offers a good number of recommendations regarding when using dupilumab should be considered.
Other Key Points:
“Dupilumab can be considered as first-line therapy in patients presenting with severe EoE”and in patients with multiple atopic diseases.
In addition, it recommends “performing a repeat EGD, along with obtaining biopsies, 5 to 6 months after either starting dupilumab therapy or whenever adjusting the dupilumab dose.” In some cases, like stricture dilatation, the authors indicate that earlier EGD may be appropriate.
The advantages/disadvantages of current treatment options are summarized in Table 3. For dupiliumab, the disadvantages include its high price of dupilumab and weekly injections. Conjunctivitis has been an adverse effect identified in its usage with other indications.
My take: Dupilumab is a major advance for patients with EoE. Due to the need for weekly injections and its costs, it is likely a 2nd line agent for most kids with EoE.
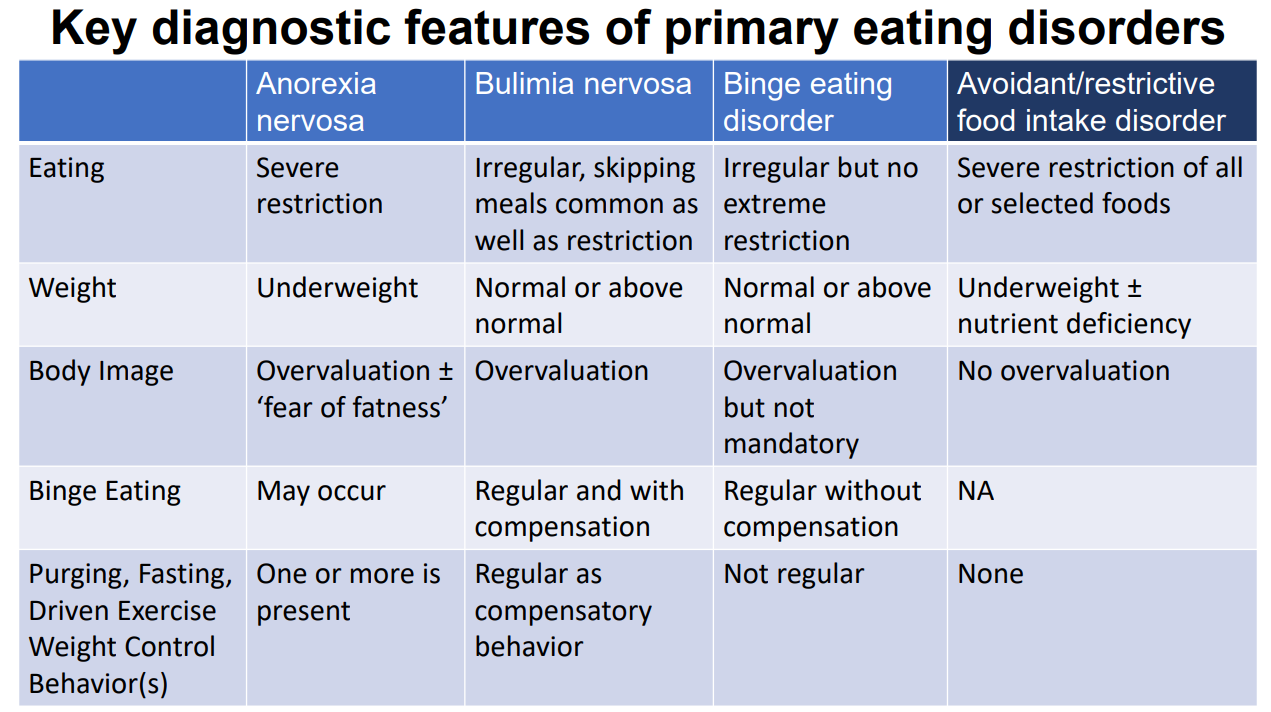
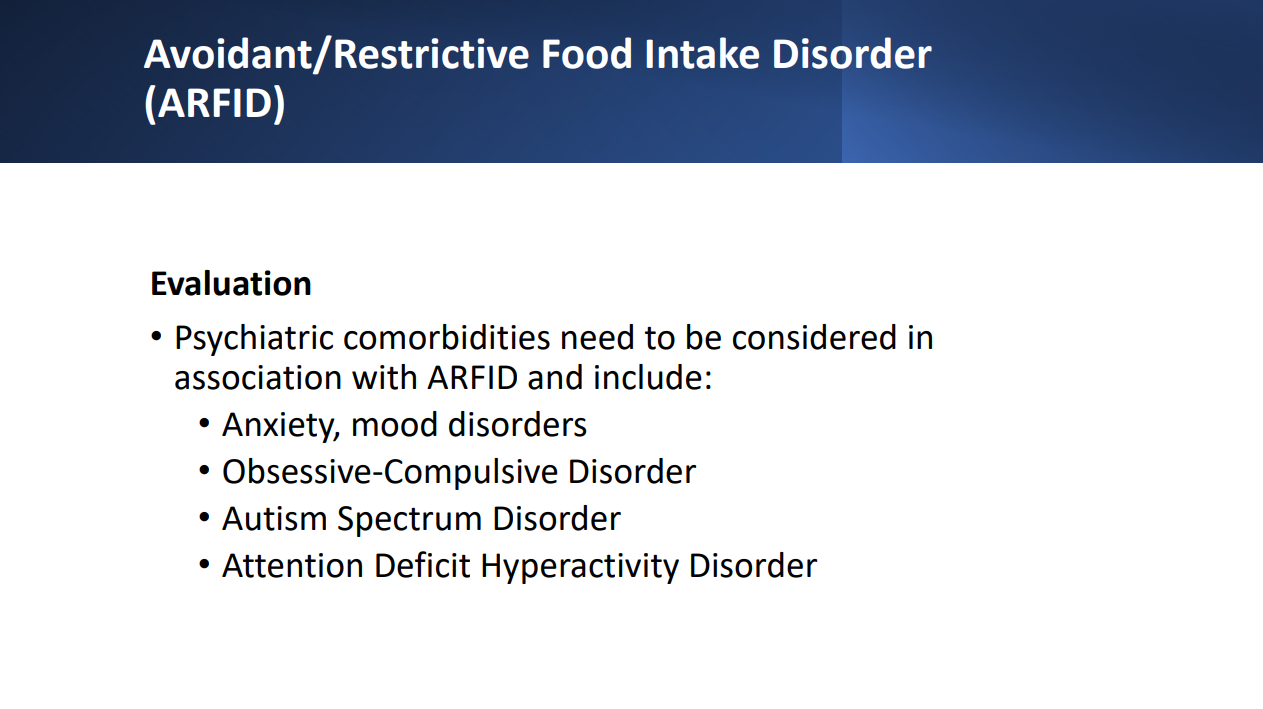
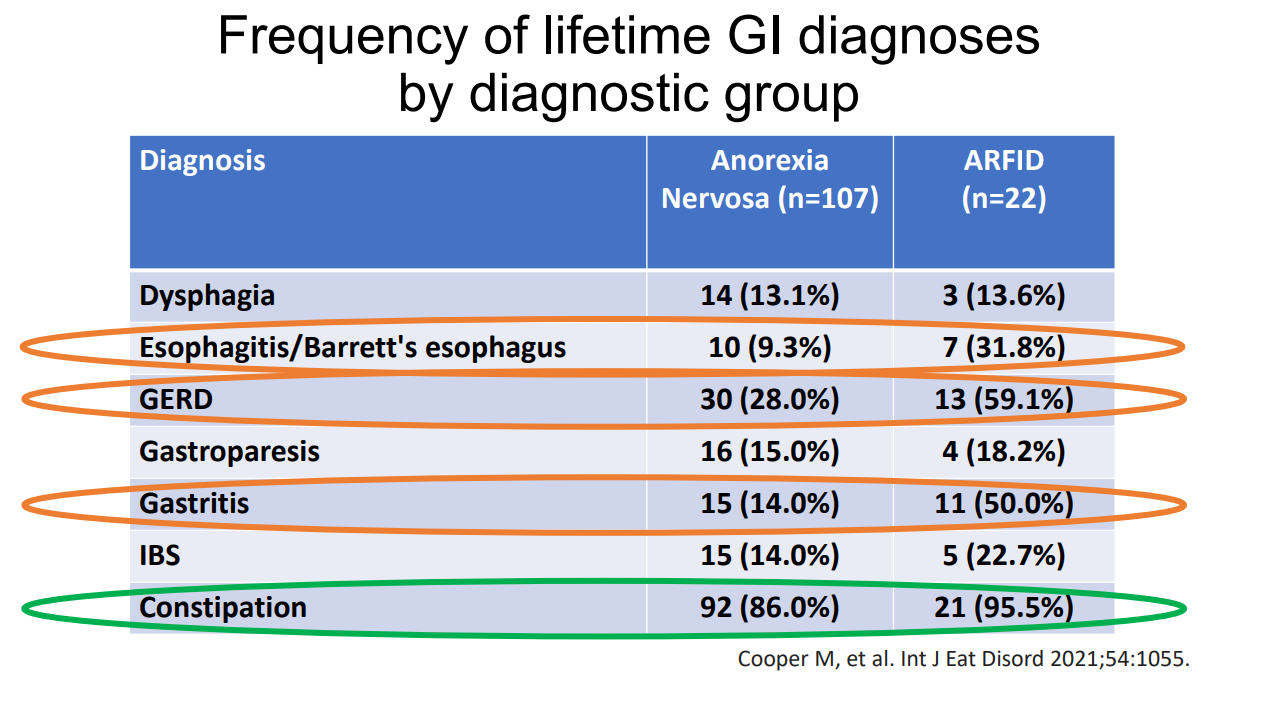
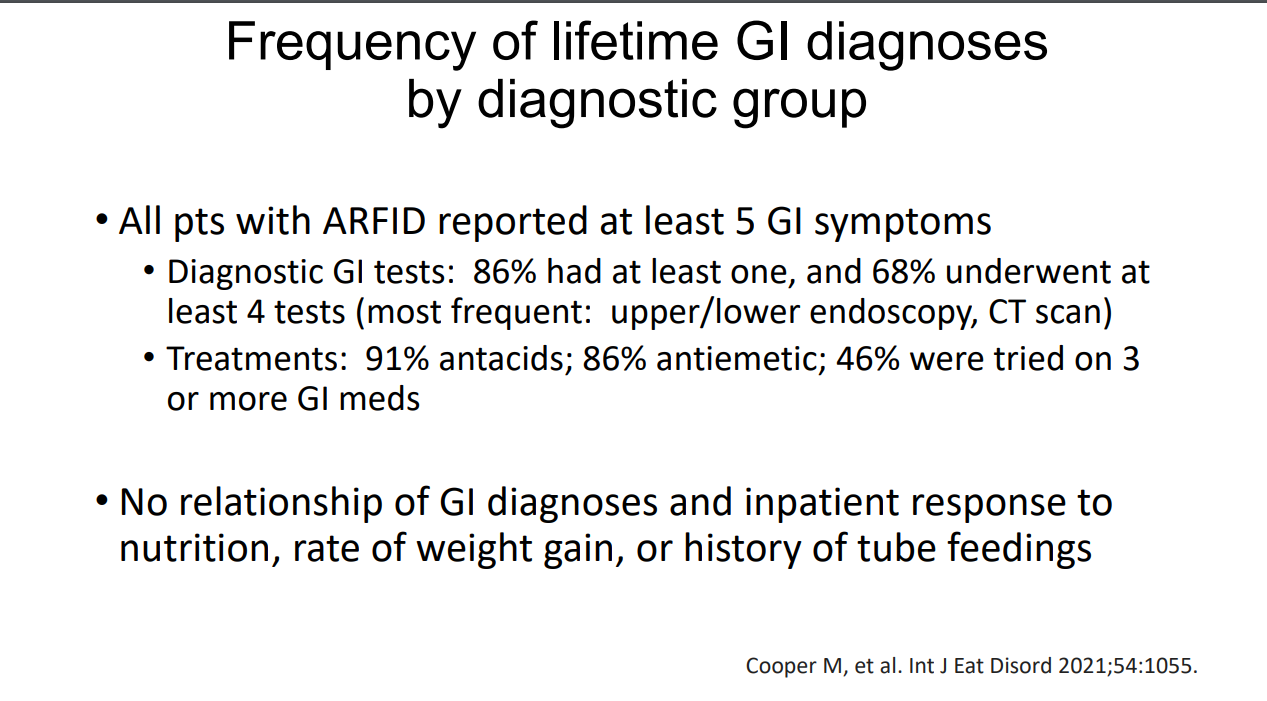
Recently, at the Georgia AAP Pediatrics by the Sea meeting, Mel Heyman presented a terrific lecture reviewing ARFID. This lecture delved into the historical backgrounds of eating disorders and described the subtypes of ARFID along with evaluation/management. This lecture was presented in honor of Stan Cohen who recently retired from our group. Here are many of the slides:
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
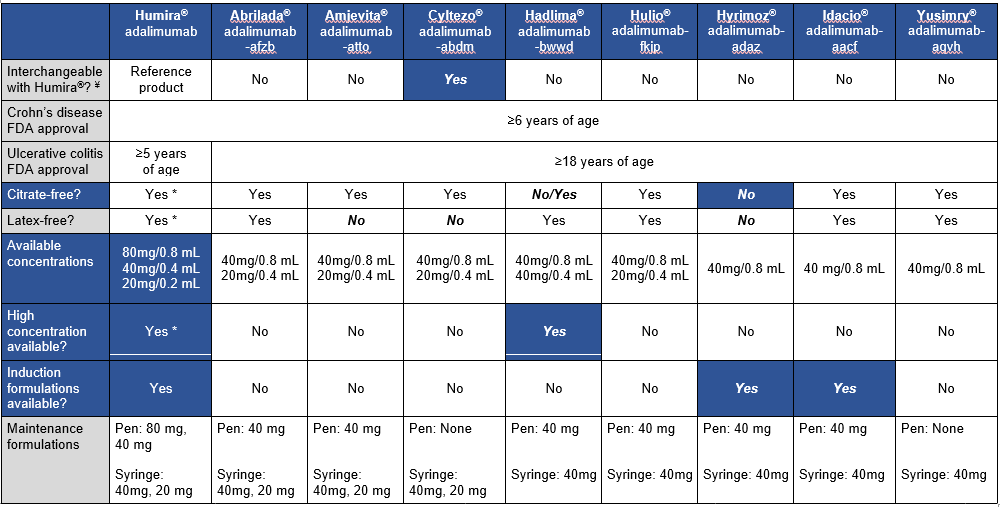
This article is a very handy update on approved adalimumab biosimilars, though even more biosimilars are expected to become available soon. The table below which is similar to a table in the article outlines the similarities and differences in these products compared to the reference product.
These biosimilars are FDA-approved for the treatment of adult and pediatric patients aged 6 and older with Crohn disease. “However, the biosimilar products are only approved for treatment of adult patients” (18 and older) with ulcerative colitis. “This may be due to the recent change in pediatric ulcerative colitis Humira FDA-approved dosing.”
My take (borrowed in part from authors): Insurance coverage decisions are likely to overlook some of these factors which are very important for pediatric patients. “The adalimumab biosimilars will likely provide a clinically effective, cost saving option for our patients, but consideration of a number of factors will be key when selecting between” them.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
#3 Currently, there is no single diagnostic tool that can conclusively identify GER as the cause of EER symptoms. Determination of the contribution of GER to EER symptoms should be based on the global clinical impression derived from patients’ symptoms, response to GER therapy, and results of endoscopy and reflux testing.
#4 Consideration should be given toward diagnostic testing for reflux before initiation of proton pump inhibitor (PPI) therapy in patients with potential extraesophageal manifestations of GERD, but without typical GERD symptoms. Initial single-dose PPI trial, titrating up to twice daily in those with typical GERD symptoms, is reasonable.
#6 In patients with suspected extraesophageal manifestation of GERD who have failed one trial (up to 12 weeks) of PPI therapy, one should consider objective testing for pathologic GER, because additional trials of different PPIs are low yield.
This commentary identifies huge gaps in our understanding of extraesophageal reflux (EER):
Clinical value of upper GI endoscopy
Diagnostic thresholds of reflux monitoring to use for EER (Is it the same as GERD?)
Significance of nonacidic or weakly acidic reflux
Whether focus should remain on distal esophageal reflux or proximal reflux
My take: If a patient has normal amounts of reflux, can they still have extraesophageal reflux symptoms? If so, how does one objectively gauge success?
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
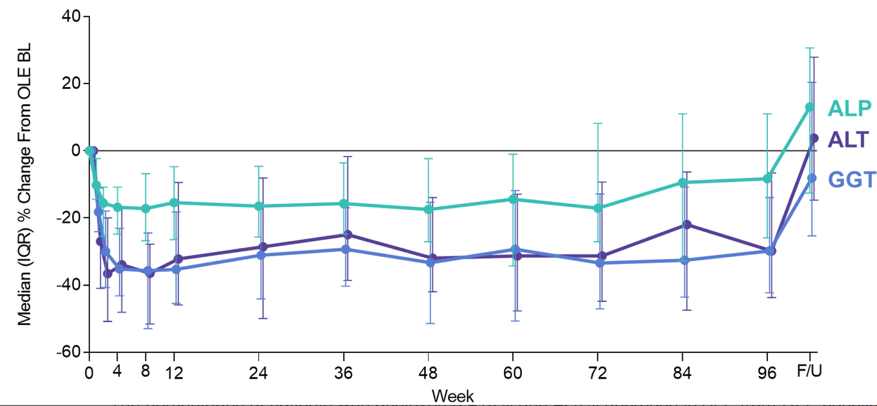
Study: There were 52 subjects enrolled in the phase II study, 47 (90%) continued in the open-label extension phase. Key findings:
At week 96, reductions in serum alkaline phosphatase (median, −8.3%), gamma-glutamyl transferase (−29.8%), alanine aminotransaminase (−29.8%), and aspartate aminotransaminase (−16.7%) occurred, and rebounded after 4 weeks of untreated follow-up. Serum cytokeratin 18 M30 and M65 (which are markers of apotopsis and necrosis)were also reduced in the OLE
My take (from authors): “Whether cilofexor impacts clinically relevant endpoints associated with PSC await the results from the placebo-controlled, phase III PRIMIS study.”
Longitudinal relative change in serum ALP, GGT, and ALT from OLE baseline to week 96 and then 4-week, untreated follow up (F/U).
This article provides a good review of the investment of private equity in gastroenterology practices. Key points:
“In addition to finding that many gastroenterologists were willing to join a PE-backed practice, PE firms found such an investment attractive because of the returns they could earn through consolidating the market.6,33…Dermatology,39 eye care,40,41 fertility,42 orthopedics,43 urology,44,45 and oncology46 are also showing increased PE activity.”
“The effects of PE ownership in gastroenterology are only recently being studied. Notable conclusions include increased costs of services, more visits by new patients, and increased esophagogastroduodenoscopy utilization absent any increase in total number of polyps or tumors removed.50…To increase revenue, one needs to increase either prices or volume of services provided, and it appears as if PE-backed practices are effectively doing both.”
“Increased volume could reflect overutilization of profitable services, unnecessary/low-value care, and/or more effective marketing, among other tactics. Higher prices could relate to more efficient charge capture, higher intensity coding, higher negotiated prices, patients being offered higher-priced services, or other causes.”
A new study finds that private equity firms own more than half of all specialists in certain U.S. markets…The medical groups were associated with higher prices in their respective markets, particularly when they controlled a dominant share, according to a paper by researchers at the Petris Center at the University of California, Berkeley, and the Washington Center for Equitable Growth, a progressive think tank in Washington, D.C. When a firm controlled more than 30 percent of the market, the cost of care in three specialties — gastroenterology, dermatology, and obstetrics and gynecology — increased by double digits...
Nearly 70 percent of all doctors were employed by either a hospital or a corporation in 2021, according to a recent analysis from the Physicians Advocacy Institute...If they could, given their rising costs and how squeezed they feel by insurers, “every independent group would want to increase its fees”…
“This builds the case for strong antitrust tools for these incrementally small but collectively larger consolidation trends,” said Erin Fuse Brown, the director of the Center for Law, Health and Society at Georgia State University.
My take: Private equity’s acquisition of medical practices is likely to drive up healthcare costs without significant improvement in patient outcomes. However, few if any other stakeholders in medical care are incentivized to provide high value care.
A previous study (SEAVUE) has suggested similar efficacy of ustekinumab and adalimumab in biologic-naive patients (post: SEAVUE: Head-to-Head Ustekimumab vs. Adalimumab) with ~60-65% clinical response at 52 weeks and ~30% endoscopic remission.
This current retrospective study sought to obtain ‘real-world’ data comparing anti-TNF agents (95 adalimumab, 61 infliximab) to ustekinumab (n=50). In the anti-TNF group, 44% (n=68) received concomitant immunomodulator therapy. Key findings:
At 3 months, clinical response rates were 86% in anti-TNF groups and 64% in the ustekinumab.
At 12 months, in adjusted multivariate analysis, clinical remission (based on Harvey-Bradshaw Index) was independently associated with the biological therapy received (odds ratio, 2.6 for anti-TNF agent vs ustekinumab;P = .02).
“In our sensitivity analysis, a significant difference in terms of efficacy was only found between infliximab and ustekinumab.”
In those with ileocolonoscopy, endoscopic healing was similar (between 6-18 months): 58% of anti-TNF group and 61% of ustekinumab group.
2% of patients in the anti-TNF group had severe adverse events compared to none in the ustekinumab group; among patients receiving adalimumab, 1 patient had cerebral aspergillosis, 1 had a postinfectious macrophage activation syndrome, and 1 had severe folliculitis needing abscess drainage.
Drug persistence at 12 months was 87% in anti-TNF group and 88% in ustekinumab group.
The discussion notes that ‘real-world’ data is important as only ~30% of patients in a regular practice would fulfill the criteria to be included in clinical trials. However, in this retrospective (non-randomized) study, there were differences in the patient population that could affect response to treatment, including a higher rate of smokers in the anti-TNF group (29% compared to 12% in the ustekinumab group).
My take: While anti-TNF therapy, particularly infliximab, may be a little better based on clinical remission, the most objective marker of efficacy, endoscopic healing, was similar. Thus, it is not clear if anti-TNF therapy is more effective than ustekinumab. To achieve optimal results, many in the anti-TNF group received immunomodulator cotherapy and dose escalation.
Joel Andres, Chef & Philanthropist, World Central Kitchen
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
The pooled placebo response rate was 29.3% (95% CI, 23.7%–35.2%) in 23 trials (n=1011)
Pooled placebo response rates were higher in idiopathic compared with diabetic gastroparesis (34.2% vs 28.1%).
Pooled responses were also higher in RCTs of shorter duration (<4 weeks, 32.6% vs ≥9 weeks, 23.2%) and in trials that did not use validated symptom questionnaires (31.2% vs 27.4%)
Adverse events occurred in 33.8% (95% CI, 26.4%–41.8%) of patients with placebo, in 27 trials, and were less common in idiopathic compared with diabetic gastroparesis (17.9% vs 43.4%)
My take: The relatively high placebo response joins the list of factors which make the management of gastroparesis difficult. This list includes trouble with diagnosis/variable results with gastric emptying studies and limited response to current treatments.