It is well-recognized that genetic mutations that persist often confer some advantages. For example, sickle cell trait (but not disease) provides protection against malaria.
A recent study shows potential health benefits in those with sucrase-isomaltase deficiency: MK Andersen, L Skotte, E Jorsboe et al. Gastroenterol 2022; 162: 1171-1182. Open Access: Loss of Sucrase-Isomaltase Function Increases Acetate Levels and Improves Metabolic Health in Greenlandic Cohorts
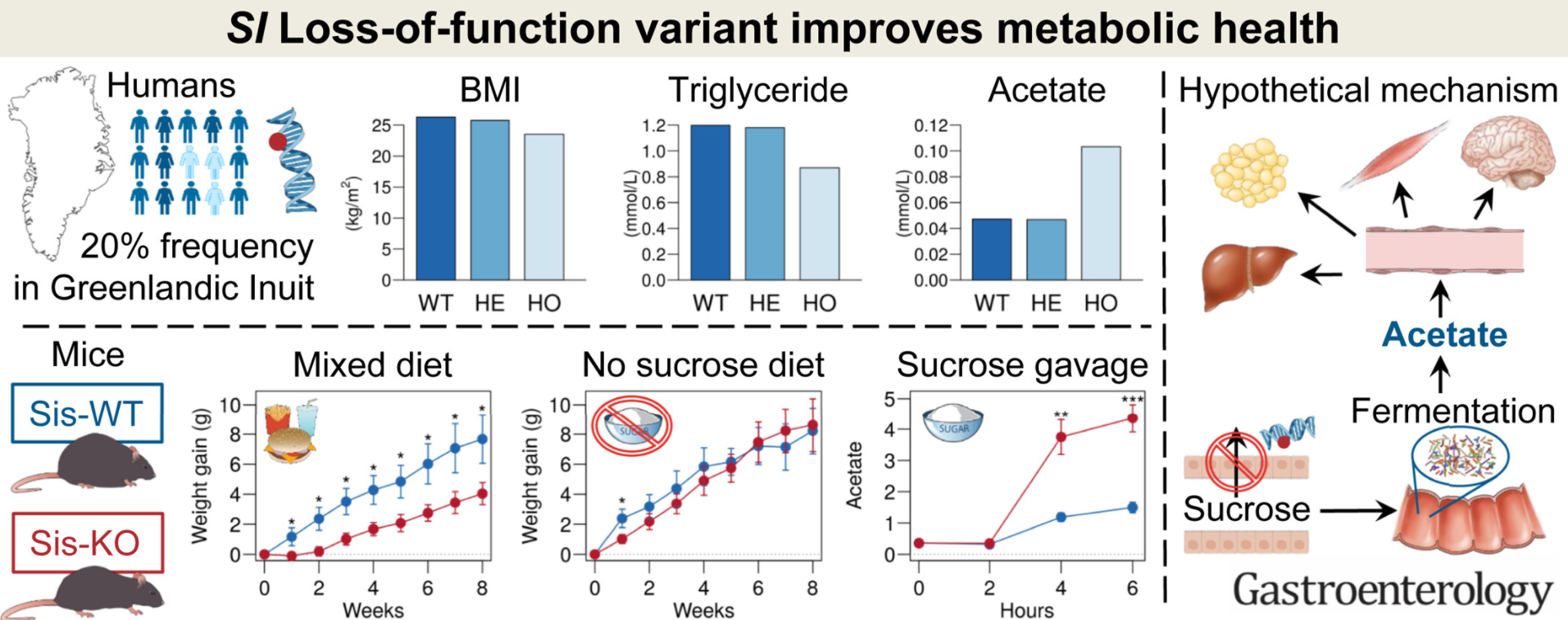
Methods: “The association between c.273_274delAG and phenotypes related to metabolic health was assessed in 2 cohorts of Greenlandic adults (n = 4922 and n = 1629). A sucrase-isomaltase knockout (Sis-KO) mouse model was used to further elucidate the findings”
Key findings:
- Homozygous carriers of the variant had a markedly healthier metabolic profile than the remaining population, including lower body mass index ( –2.0 kg/m2; P = 3.1 × 10–5), body weight (–4.8 kg; P = 5.1 × 10–4), fat percentage (–3.3%; P = 3.7 × 10–4), fasting triglyceride (–0.27 mmol/L; P = 2.3 × 10–6), and remnant cholesterol (–0.11 mmol/L; P = 4.2 × 10–5).
- The metabolic profile “was likely mediated partly by higher circulating levels of acetate observed in homozygous carriers” (0.056 mmol/L; P = 2.1 × 10–26), and partly by reduced sucrose uptake, but not lower caloric intake.
- “These findings were verified in Sis-KO mice, which, compared with wild-type mice, were leaner on a sucrose-containing diet, despite similar caloric intake, had significantly higher plasma acetate levels in response to a sucrose gavage, and had lower plasma glucose level in response to a sucrose-tolerance test.”
My take: It should not be surprising that a genetic condition that results in limited sucrose intake would have health benefits. Perhaps correcting this condition will result in unexpected health issues similar to health issues that can develop in those with celiac disease after institution of a gluten-free diet (Gastroenterol 2013; 144: 912-17).
Related blog posts:
- Celiac disease and less diabetes?
- “Bowel Sounds” Pediatric GI Podcast: Dr. Martin and Dr. Vartabedian (2021)
- Lessons in Diarrhea (Part 1) 2018
- Lessons in Diarrhea (part 2) 2018
- Congenital Sucrase Isomaltase Deficiency
Graphical Abstract: