N Narula et al. Clin Gastroenterol Hepatol 2023; 21: 2483-2495. Open Access! Food Processing and Risk of Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis
JA Fitzpatrick et al. Clin Gastroenterol Hepatol 2023; 21: 2478-2480 (editorial). Open Access! Ultra-processed Foods and Risk of Crohn’s Disease: How Much is Too Much?
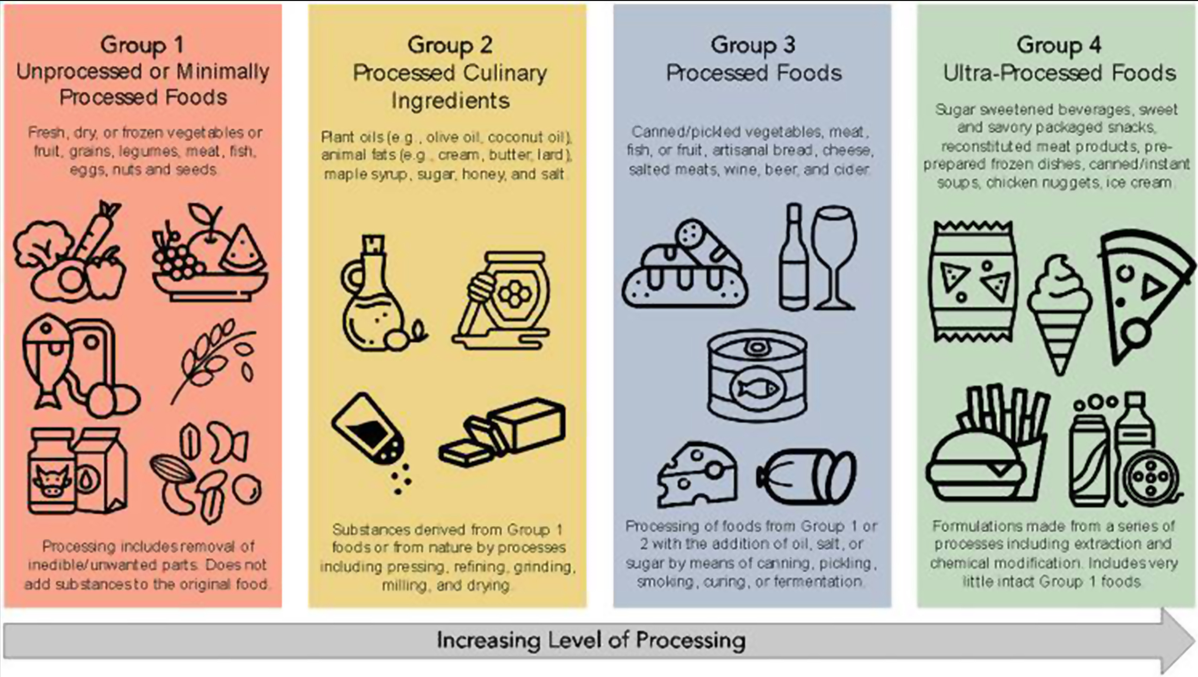
A total of 1,068,425 participants were included (13,594,422 person-years) among 5 cohort studies published between 2020 and 2022. The average age of participants ranged from 43 to 56 years. Key findings:
- Crohn’s disease: During follow-up, 916 participants developed CD, and 1934 developed UC. There was an increased risk for development of CD for participants with higher consumption of ultra-processed foods compared with those with lower consumption (HR, 1.71; 95% CI, 1.37–2.14; I2 = 0%) and a lower risk of CD for participants with higher consumption of unprocessed/minimally processed foods compared with those with lower consumption (HR, 0.71; 95% CI, 0.53–0.94; I2 = 11%).
- Ulcerative colitis: There was no significant association between risk of UC and ultra-processed foods (HR, 1.17; 95% CI, 0.86–1.61; I2 = 74%) or unprocessed/minimally processed foods (HR, 0.84; 95% CI, 0.68–1.02; I2 = 0%).

The associated editorial by Fitzpatrick et al, notes that “there are plausible mechanisms that explain the associations of higher UPFs and development of CD, such as: (1) displacing the intake of minimally processed foods and subsequently reducing exposure to beneficial micronutrients, antioxidants, and phytochemicals; (2) driving overconsumption of total calories7; and (3) increasing exposure to non-nutritive food substances that have been implicated in the development of CD in pre-clinical studies…The notion is that a lower UPF intake is better, but a cutoff value remains elusive.”8
My take (borrowed from editorial): “the population studies have indicated that the extremes of UPF intake are related to risk of CD and that such associations are underpinned by plausible biological mechanisms, suggesting causality.”
Related blog posts: