This blog entry has abbreviated/summarized this presentation. Though not intentional, some important material is likely to have been omitted; in addition, transcription errors are possible as well.
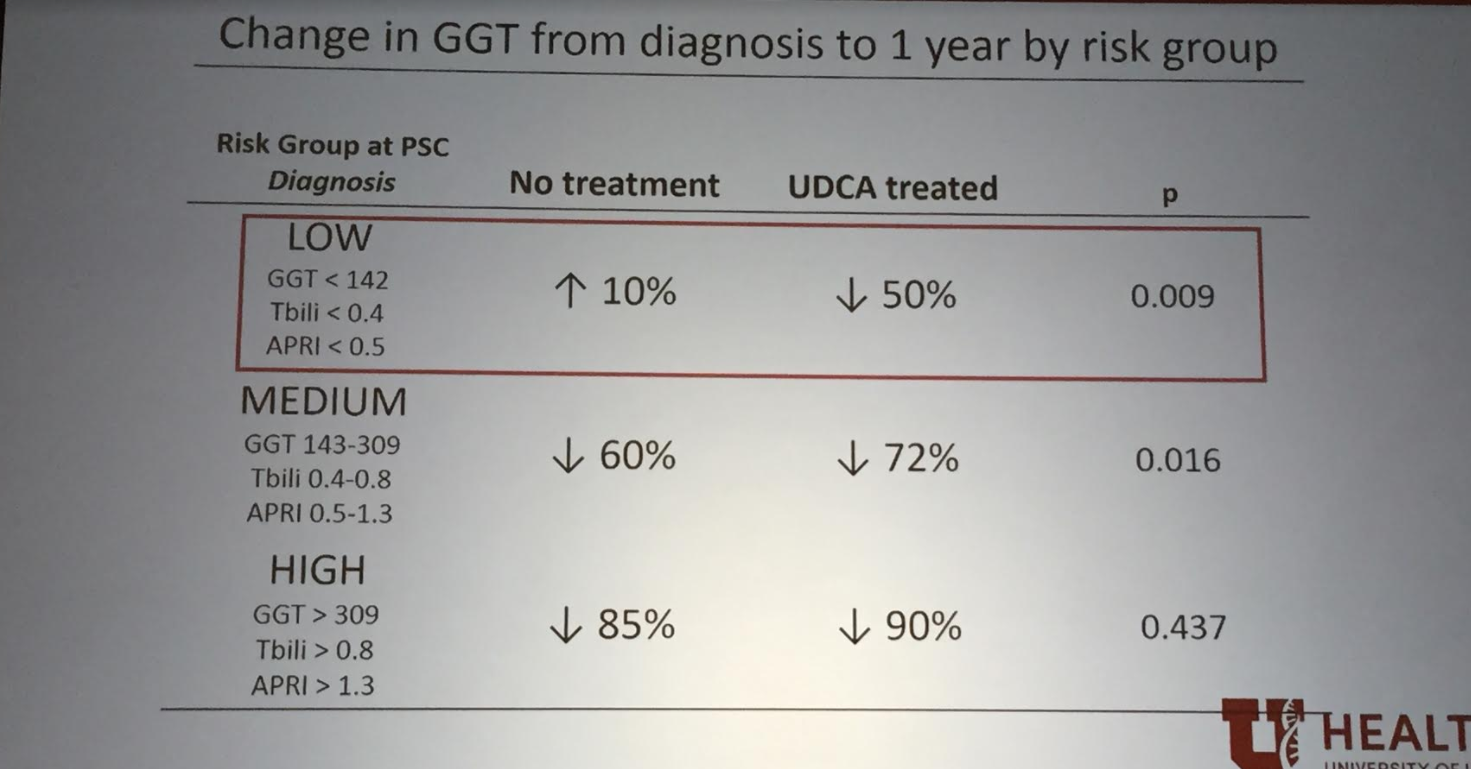
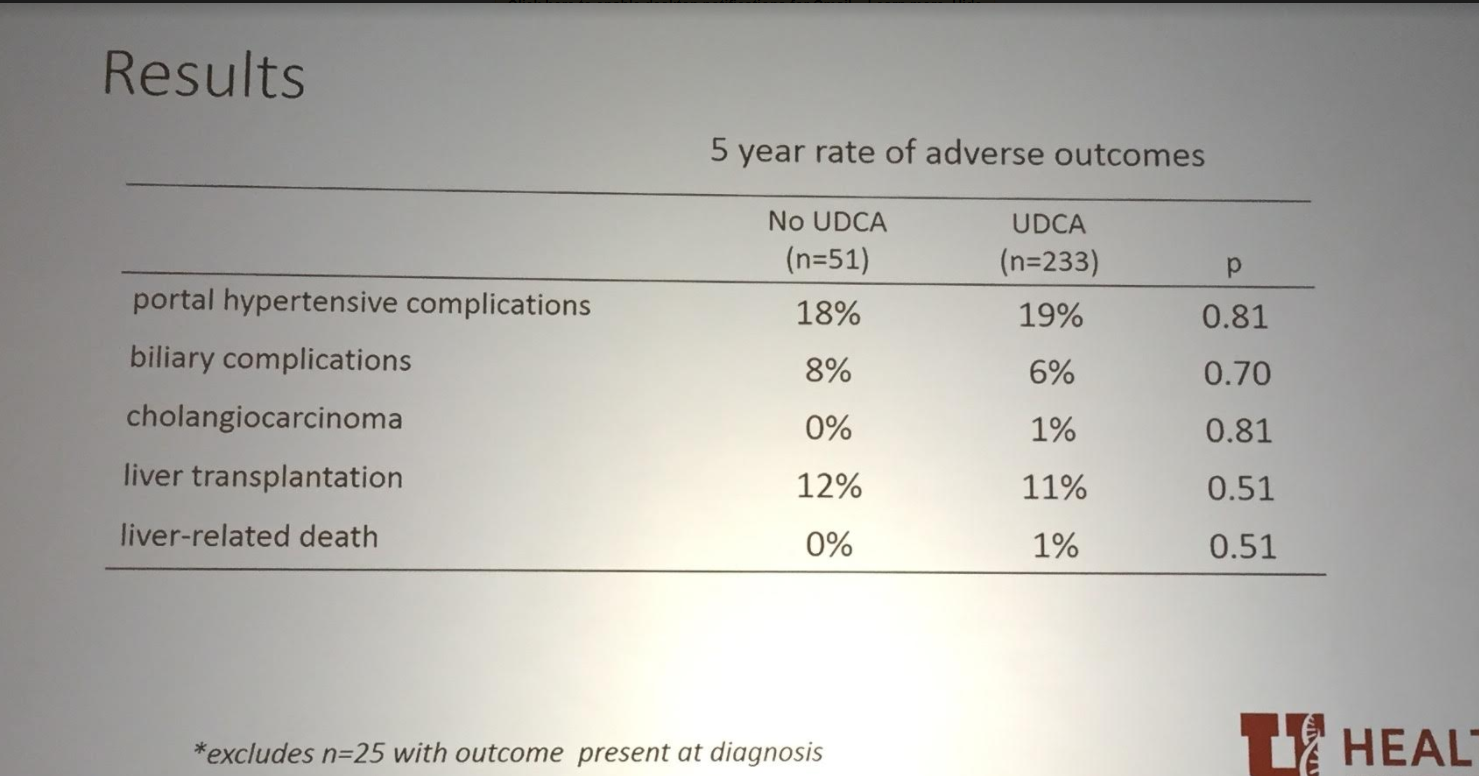
Improvement in GGT Predicts Event-free Survival in Primary Sclerosing Cholangitis Regardless of Ursodeoxycholic Acic Treatment.
Mark Deneau et al. (Grand Watkins Prize).
Key points:
- PSC is difficult to study due to its rarity and due to its slow progression; thus surrogate biomarkers are needed.
- Alkaline phosphatase is not a good biomarker in children
- GGT level at one year after diagnosis was predictive of prognosis
- Ursodeoxycholic acid does not appear to be effective






Optimizing Nutrition in Intestinal Failure
Justine Turner, University of Alberta
Key points:
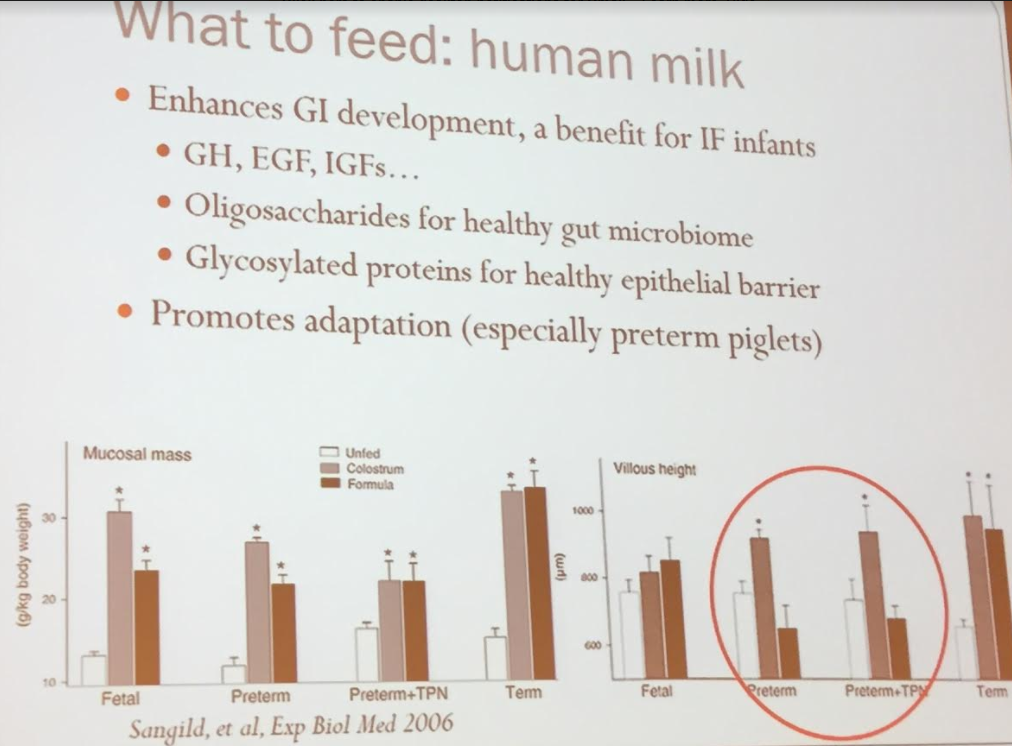
- Human milk is an ideal “formula” for infants, including those with intestinal failure
- Oral feedings are important
- Combination of bolus feeds and continuous feeds is reasonable
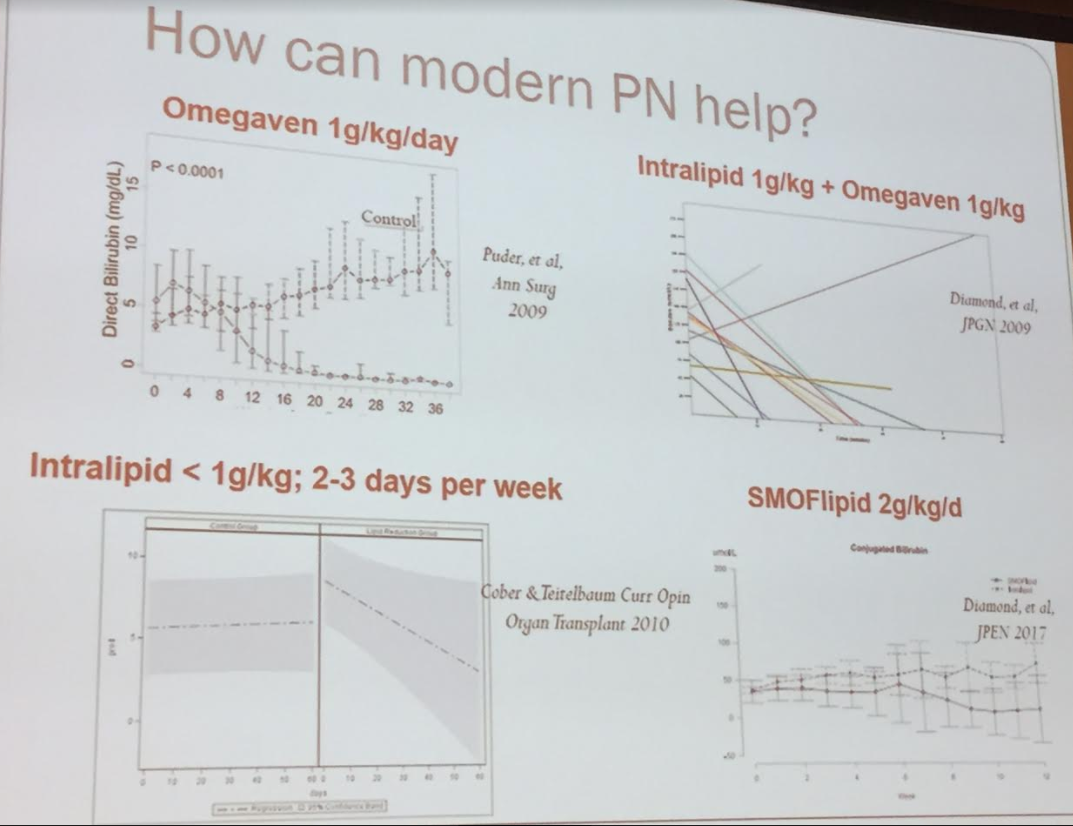
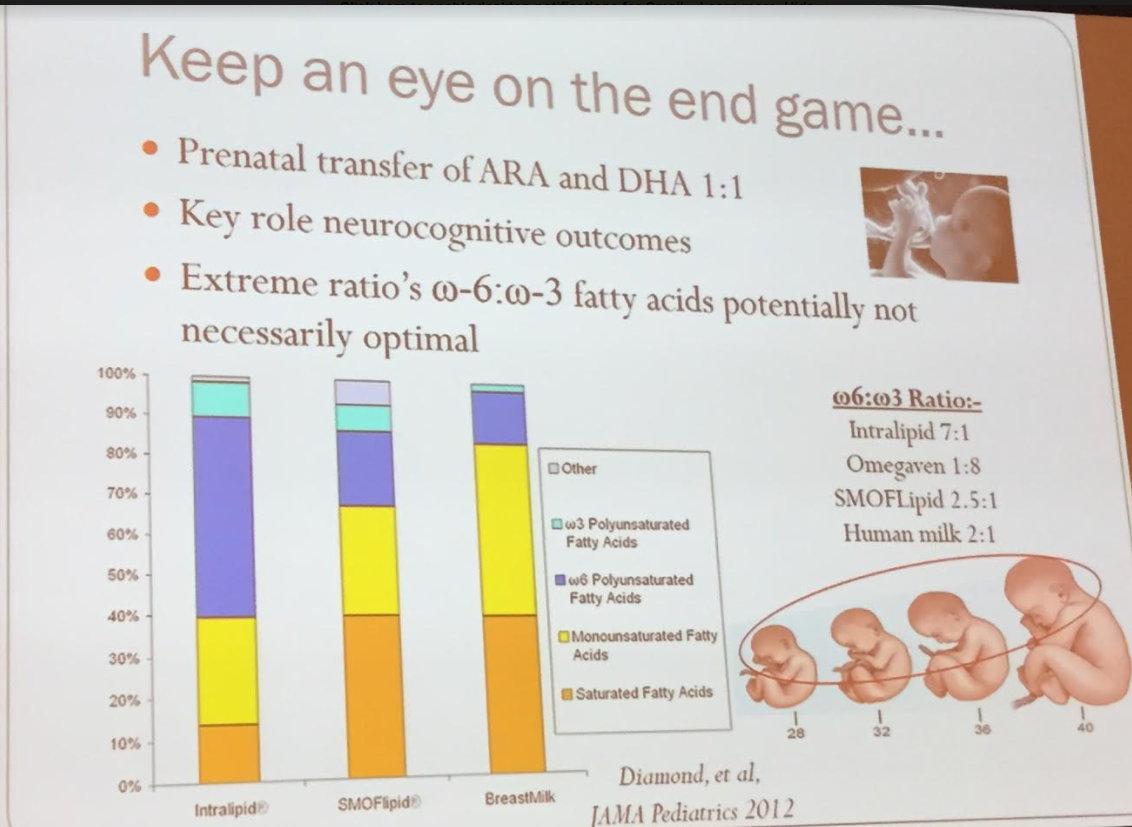
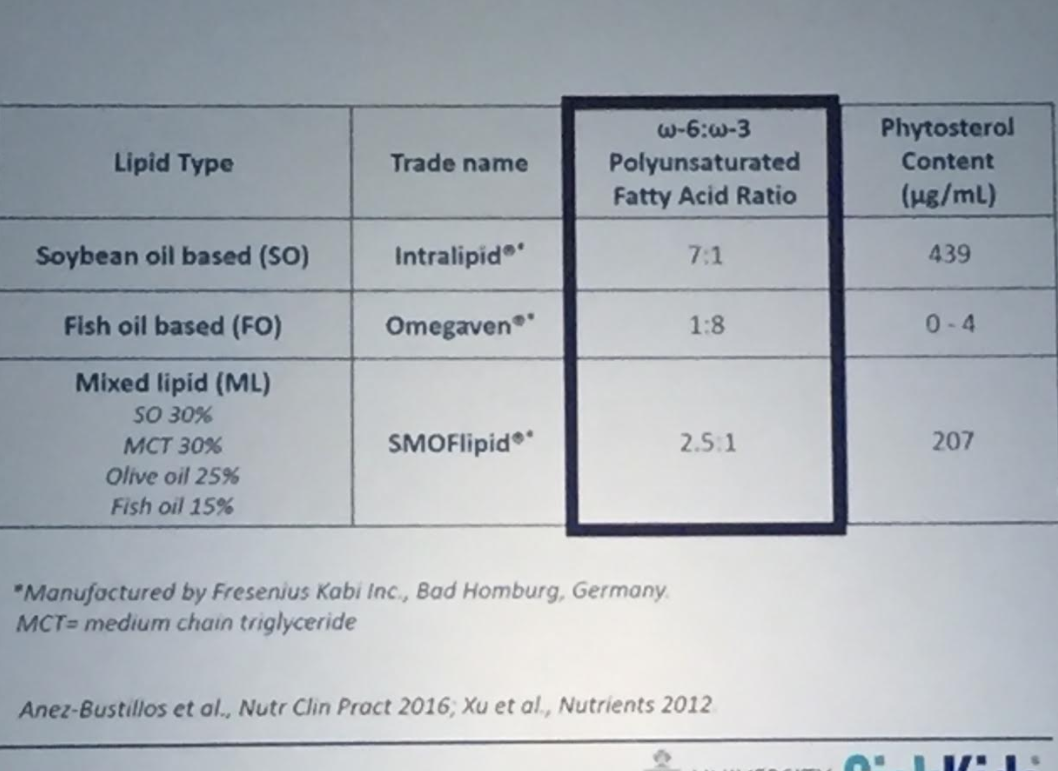
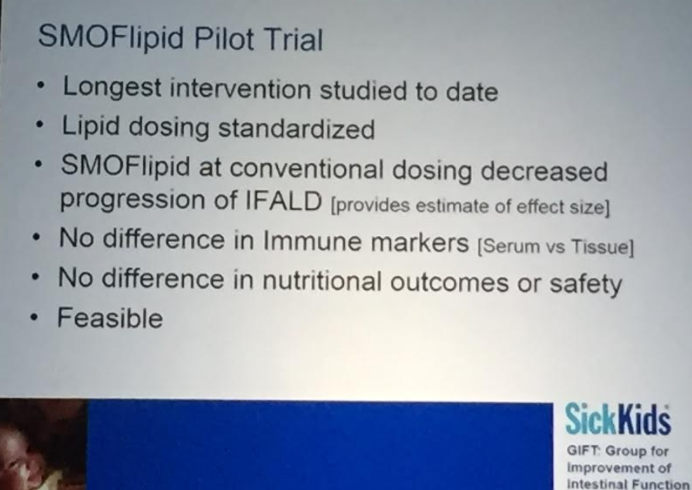
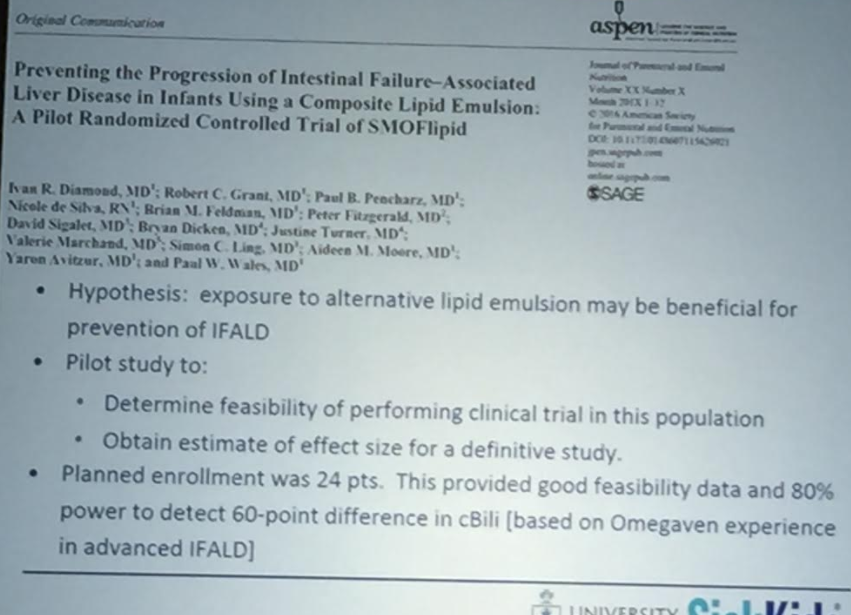
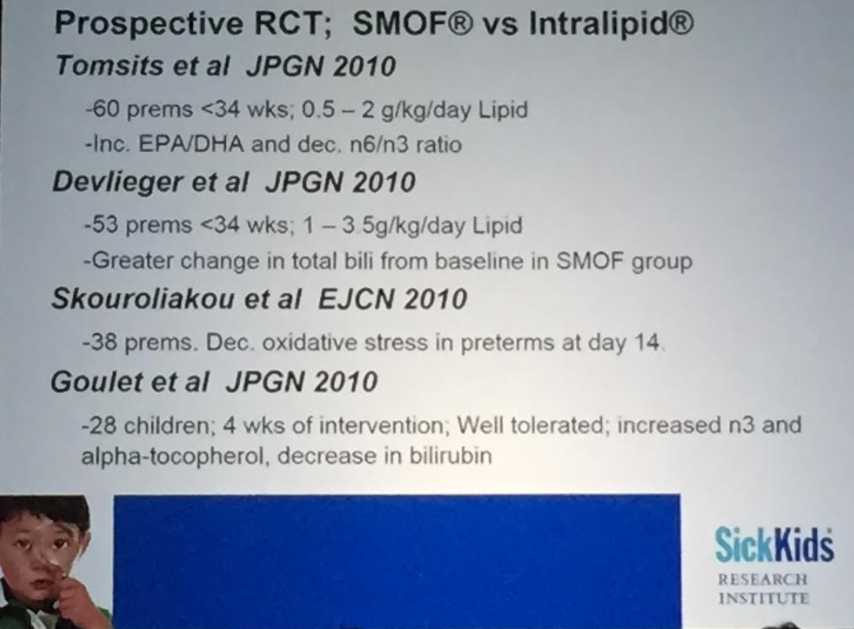
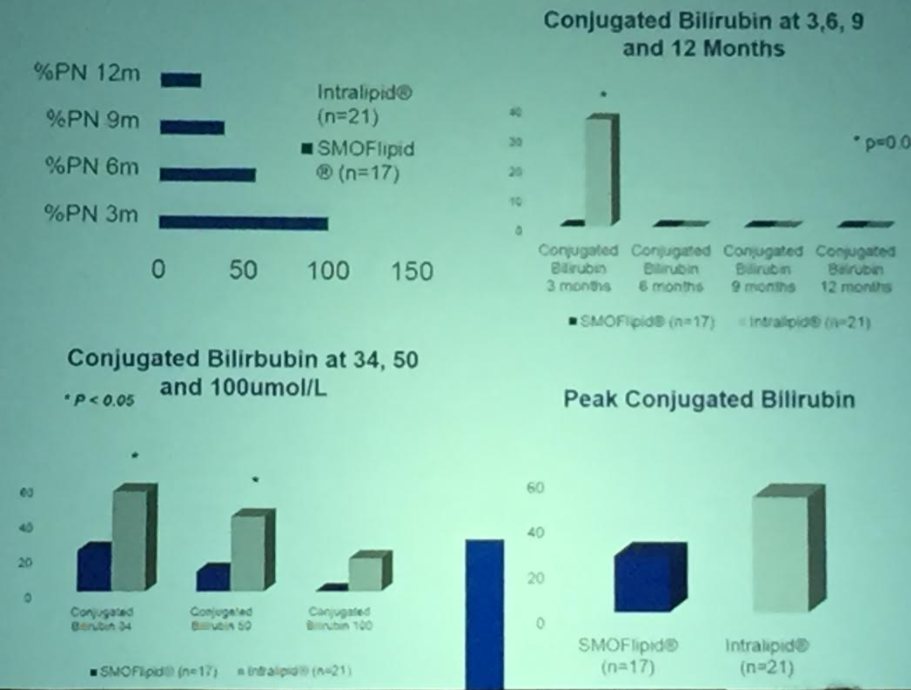
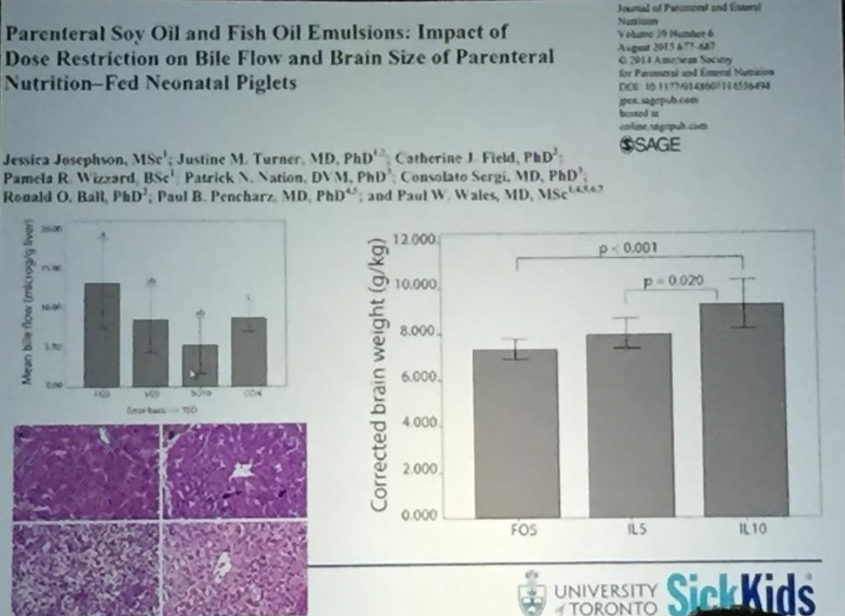
- SMOFlipid allows higher lipid dose administration without hepatoxicity; this may improve cognitive outcomes
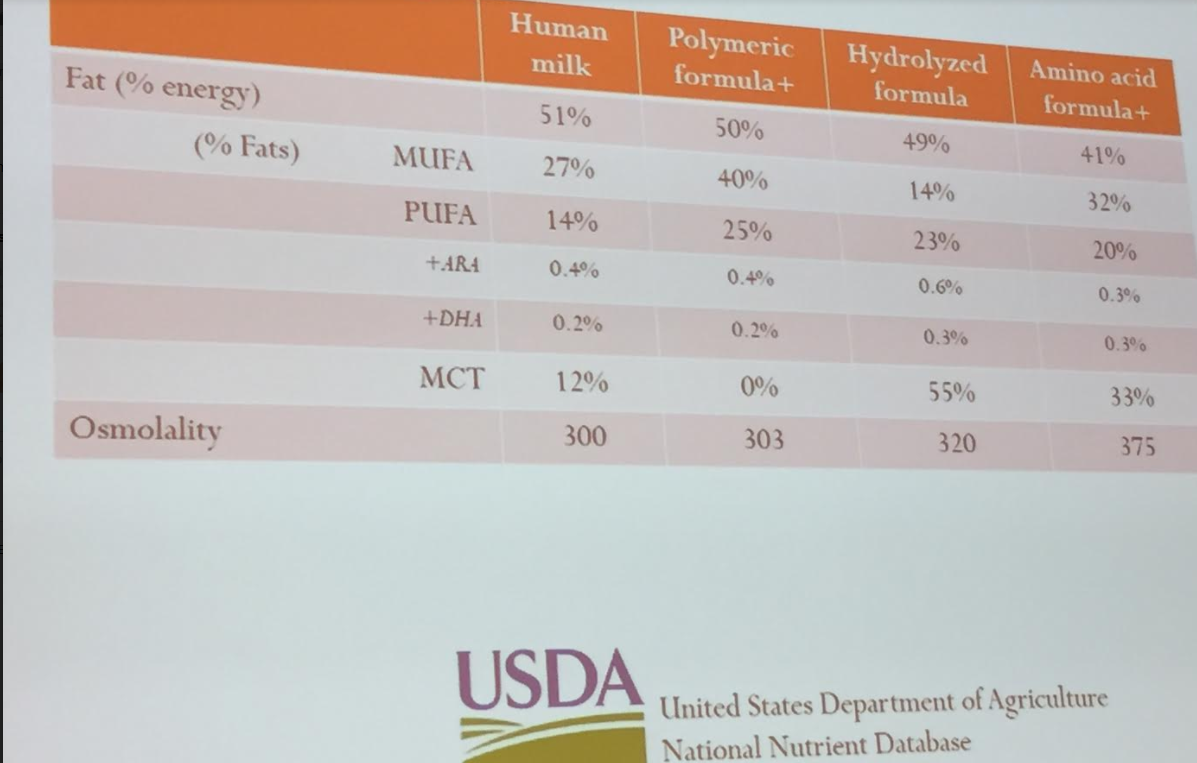
- Amino acid based formulas have higher osmolality which can contribute to diarrhea
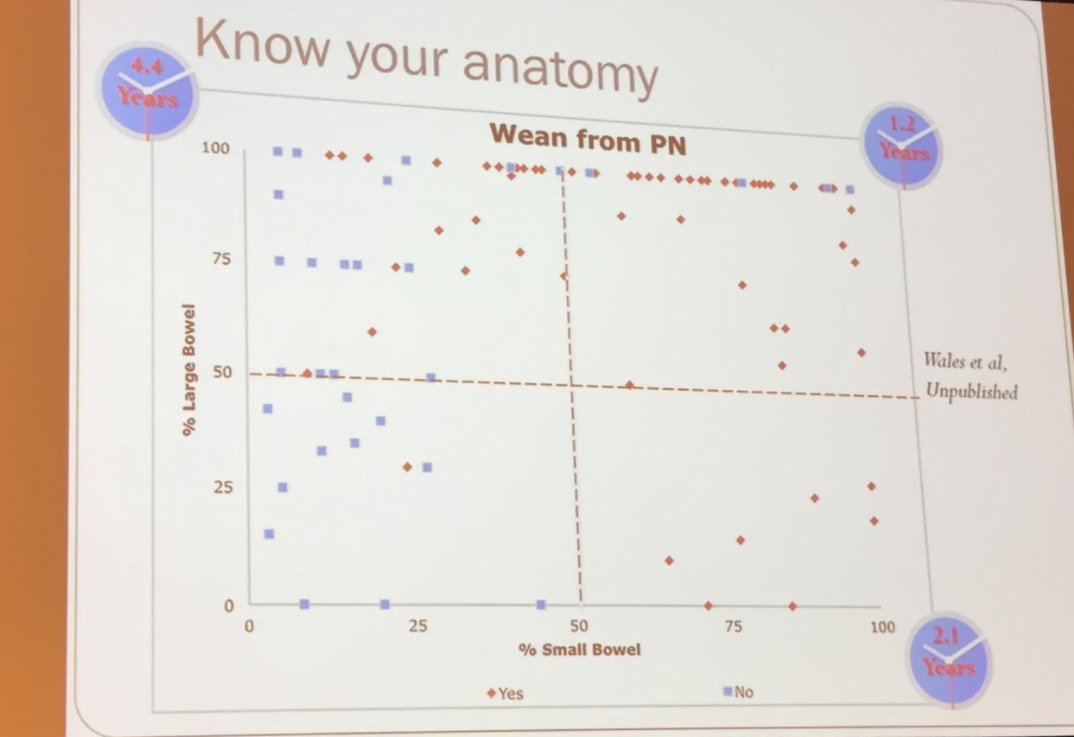
Patients with >50% of small bowel and >50% of colon were most likely to achieve enteral autonomy (GIFT registry)