This study included 9 RCTs involving a total of 445 participants. Key findings:
Though some of the study findings seemed to favor prebiotics, all evidence was of very low certainty.
“There may be no difference in occurrence of clinical relapse when adjuvant treatment with prebiotics is compared with adjuvant treatment with placebo for maintenance of remission in UC.”
“Adjuvant treatment with prebiotics may result in more total adverse events when compared to adjuvant treatment with placebo for maintenance of remission. The evidence was of low certainty.”
My take: Currently, there is no solid evidence to recommend prebiotics in patients with ulcerative colitis.
Like yesterday’s article on GTs, this is another terrific review with plenty of helpful images and advice regarding ostomy management.
Background: “There are upwards of 1 million people living with ostomies (ostomates) in the United States.” “Approximately 75% of all ostomies in the pediatric population are created in the neonatal or infant patient.”
Table 1 lists the purposes and types of ostomies including gastrostomy, jejunostomy, ileostomy, appendicostomy (Malone), cecostomy, colostomy and urinary diversions (eg. Mitrofanoff).
Surgical considerations are reviewed including optimizing nutrition preoperatively and minimizing corticosteroids. Biologics: “The most recent evidence does not support a delay in gastrointestinal surgery for children with IBD receiving biological therapy…[and] typically, biological therapy can be resumed 14 to 28 days after the operation.” For oral small molecules (with short half-lives), these may be restarted sooner if indicated.
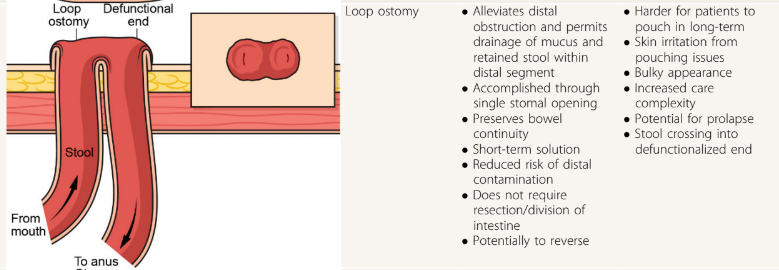
Table 2 provides pictures of the lower ostomies. For example:
Postoperative care is discussed including healing times, need for wound ostomy nurse input, and addressing self-image. Patients with motility disorders are “more likely to experience postoperative complications”
Table 4 details the products for pouch care including pouching systems, skin barriers, pouch liner, gas vent, pouch lubricant, pouch covers, and adhesive remover.
Table 5 summarized ostomy-related complications and treatments. Complications include stomal necrosis, stomal bleeding, stomal retraction, mucocutaneous separation, parastomal hernia, stoma prolapse (can apply cool compresses, apply osmotic agent (sugar) or manually reduce), stoma stenosis, and dermatitis.
Table 6 addresses medical management issues like odor, blockage, diarrhea, and constipation. This table also provides recipes for antegrade enemas (see below) and links including a very useful bowel management guide for families (28 pg from Boston Children’s) and enema ingredients and supplies (2 pg from Seattle Children’s); the latter has some overlapping information with the former.
At the conclusion of the article, there is further discussion of systemic and ostomy-related complications (much of which is summarized in Table 5). The article references the Ostomy Skin Tool as a metric to follow the clinical state of the ostomy. The United Ostomy Associations of America (ostomy.org) is listed as a good resource (which it is!).
My take: This is a very useful resource. Even a quick read will make clinicians appreciative of having the assistance wound ostomy nurses.
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
Dr. Joel Rosh gave our group an excellent update on sequencing therapy for ulcerative colitis (UC). My notes below may contain errors in transcription and in omission. Along with my notes, I have included many of his slides.
There are only two FDA-approved biologics in pediatric Ulcerative Colitis. It typically takes 8-10 years for a medication with approval in adults to receive FDA approval in children
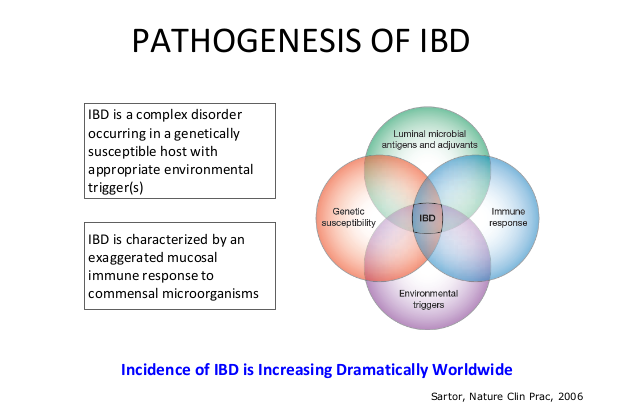
The concept of IBD as two diseases, Crohn’s disease and UC, is flawed; there are more than 200 susceptibility genes for inflammatory bowel disease
There has been an increasing incidence and prevalence of IBD. Some of this increase is likely due to our diet and its effects on the microbiome
Ultrasound is a nice tool to see what is going on in real time and shows that UC is really a transmural disease. UC changes in the bowel can result in fibrosis
Consider cytokine-basis for disease as a way to conceptualize disease presentation compared to organ-based disease. Many autoimmune diseases (eg. JIA, RA, Psoriasis) are different manifestations related to cytokine-based autoimmunity
Almost all pediatric IBD can be considered higher risk based on known risk factors including disease extent (>80% of pediatric UC is pancolitis) and disease age of onset
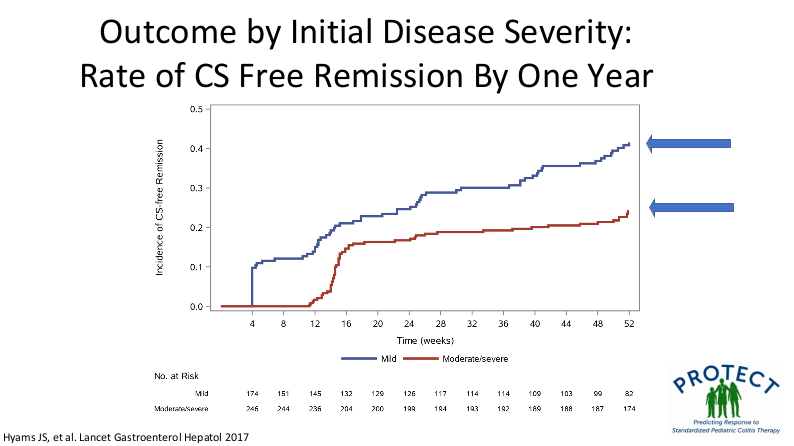
Mesalamine steroid-free clinical remission rates are about 1/3rd after 1 year of treatment
Overall, there has been an improvement in colectomy rates since 2001; there still appears to be a bump in the colectomy rate after having UC for more than 10 years
Elevated CRP is less common in patients with UC, compared to Crohn’s disease, and is a marker for more severe disease activity
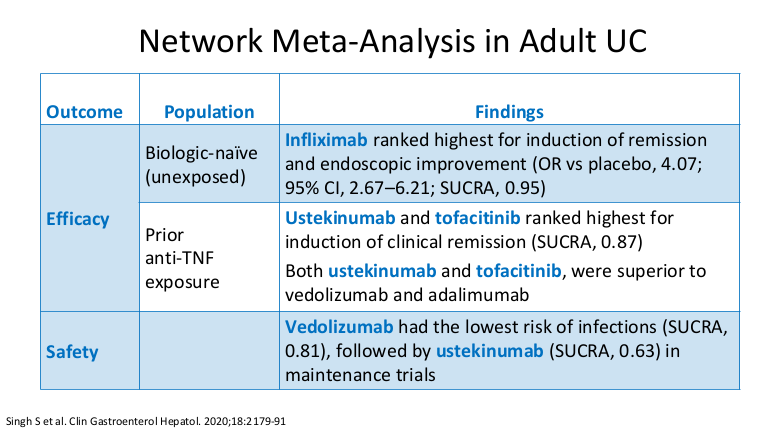
Dr. Rosh prefers to avoid some terms including biologic-naive and steroid failure; he favors biologic-unexposed for the former. For the latter, he tries to make it clear that the patient was not a steroid failure. Steroids failed the patient rather than the patient failing the steroids
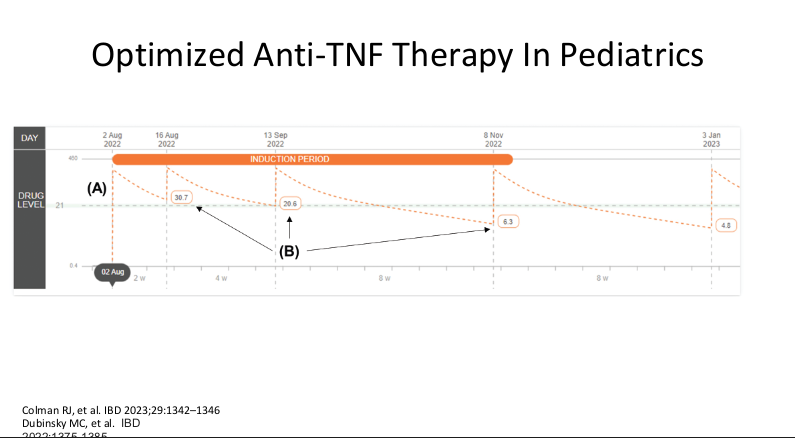
Therapeutic drug monitoring (TDM) is mainly beneficial for anti-TNF agents at this time. Use of TDM can help monotherapy achieve similar results as combination therapy. For infliximab, Dr. Rosh’s ‘rule of thumb’ is 28-18-8 for 2 week trough, 6 week trough, and maintenance trough. Therapeutic levels will meet or exceed these trough levels.
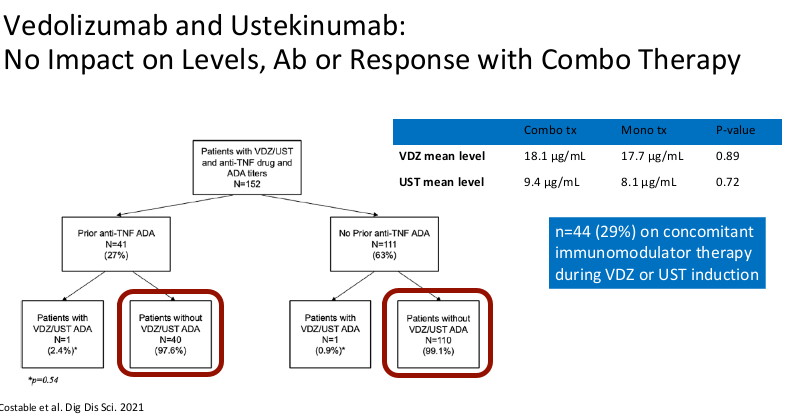
Combination therapy has not been shown to improve pharmacokinetics for vedolizumab or ustekinumab
Generally, a washout period is not needed when changing biologic therapies. In fact, having some overlap in the medications may have some therapeutic benefit
Upadacitinib (Rinvoq) appears to be the most effective JAK for IBD. It is labelled for use as a 2nd-line agent but may be superior for some sicker patients. Rinvoq could be considered as a ‘bridge’ medication in patients with acute severe ulcerative colitis with transition to another biologic like vedolizumab
It is important for families to be informed that there is a black box warning for the use of JAK inhibitors. However, major cardiac adverse events (MACE) do not appear to be increased in patients without preexisting cardiac disease risk factors
Disclaimer: This blog, gutsandgrowth, assumes no responsibility for any use or operation of any method, product, instruction, concept or idea contained in the material herein or for any injury or damage to persons or property (whether products liability, negligence or otherwise) resulting from such use or operation. These blog posts are for educational purposes only. Specific dosing of medications (along with potential adverse effects) should be confirmed by prescribing physician. Because of rapid advances in the medical sciences, the gutsandgrowth blog cautions that independent verification should be made of diagnosis and drug dosages. The reader is solely responsible for the conduct of any suggested test or procedure. This content is not a substitute for medical advice, diagnosis or treatment provided by a qualified healthcare provider. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a condition.
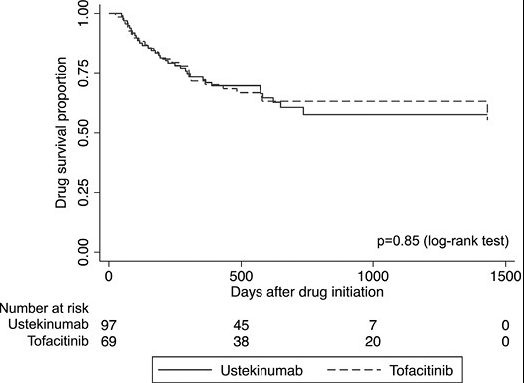
In this real-world cohort of anti-TNF-exposed patients with ulcerative colitis, tofacitinib (n=69) and ustekinumab (n=97) demonstrated similar effectiveness in achieving steroid-free clinical remission (SCFR) at 12 and 52 weeks. The median follow-up was 88.0 and 62.0 week, respectively. 35 of 66 in the tofacitinib cohort had dose reduction from the starting dose of 10 mg twice daily. This reduction occurred at a mean of 144 days. 59 of 97 in the ustekinumab cohort received either Q4W dosing (n=43) or Q6W (n=16).
Key findings:
53% of patients receiving tofacitinib and 32% of patients receiving ustekinumab achieved SFCR at 12 weeks. Tofacitinib-treated patients had higher baseline Mayo endoscopic subscores and CRPs.
At 52 weeks, approximately 50% of patients in both treatment groups achieved SFCR. There were also high proportions (>60%) of patients in both treatment groups who had endoscopic response within 52 weeks.
Both drugs were well-tolerated, as only 1 patient in each treatment group discontinued therapy due to an AE during >260 patient-years of follow-up.
My take: This shows similar response to either tofacitinib and ustekinumab in a cohort that had refractory disease as patients were anti-TNF failures and most had prior vedolizumab as well.
There are 12 “best practice” recommendations. Here are a few of them:
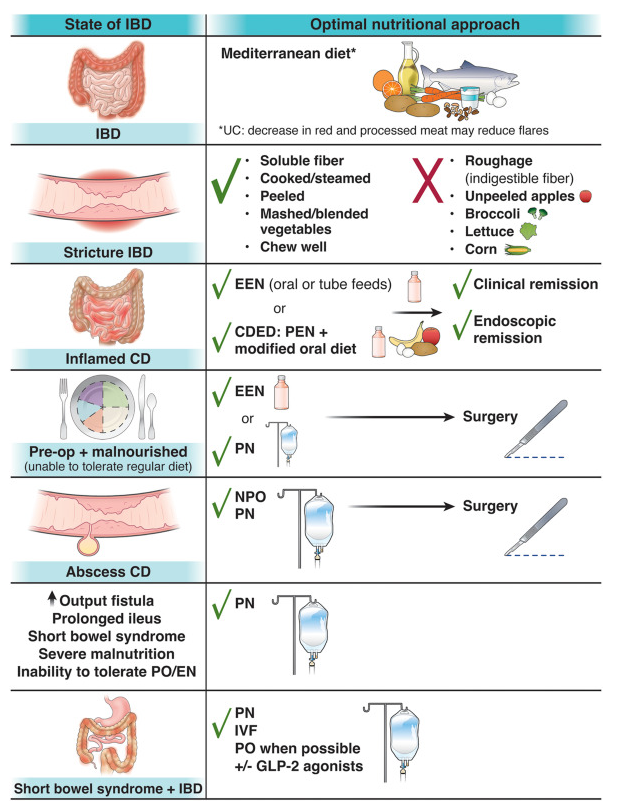
Best Practice Advice 1: Unless there is a contraindication, all patients with IBD should be advised to follow a Mediterranean diet rich in a variety of fresh fruits and vegetables, monounsaturated fats, complex carbohydrates, and lean proteins and low in ultraprocessed foods, added sugar, and salt for their overall health and general well-being. No diet has consistently been found to decrease the rate of flares in adults with IBD. A diet low in red and processed meat may reduce ulcerative colitis flares, but has not been found to reduce relapse in Crohn’s disease.
Best Practice Advice 3: Exclusive enteral nutrition using liquid nutrition formulations is an effective therapy for induction of clinical remission and endoscopic response in Crohn’s disease, with stronger evidence in children than adults. Exclusive enteral nutrition may be considered as a steroid-sparing bridge therapy for patients with Crohn’s disease.
Best Practice Advice 6: In patients with IBD who have an intra-abdominal abscess and/or phlegmonous inflammation that limits ability to achieve optimal nutrition via the digestive tract, short-term parenteral nutrition may be used to provide bowel rest in the preoperative phase to decrease infection and inflammation as a bridge to definitive surgical management and to optimize surgical outcomes.
Best Practice Advice 7: We suggest the use of parenteral nutrition for high-output gastrointestinal fistula, prolonged ileus, short bowel syndrome, and for patients with IBD with severe malnutrition when oral and enteral nutrition has been trialed and failed or when enteral access is not feasible or contraindicated.
Best Practice Advice 10: All patients with IBD should be monitored for vitamin D and iron deficiency. Patients with extensive ileal disease or prior ileal surgery (resection or ileal pouch) should be monitored for vitamin B12 deficiency.
Best Practice Advice 12:Breastfeeding is associated with a lower risk for diagnosis of IBD during childhood. A healthy, balanced, Mediterranean diet rich in a variety of fruits and vegetables and decreased intake of ultraprocessed foods have been associated with a lower risk of developing IBD.
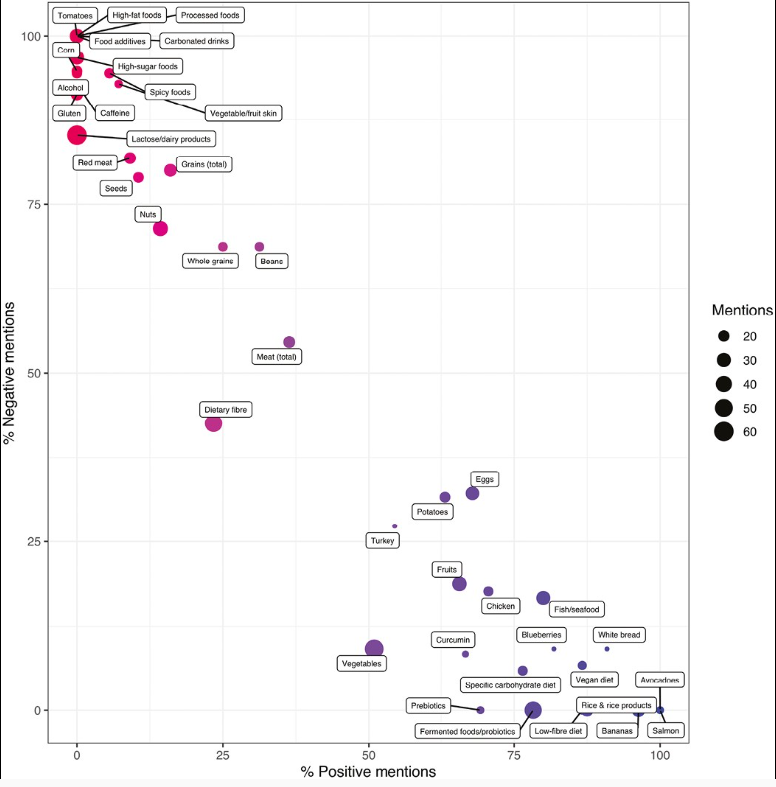
The authors assessed videos discussing dietary aspects (food, diet-related items, and advisory comments [FODRIACs]) on YouTube. Of 1800 videos screened, a total of 160 were included in the final analysis.
Background: “Currently, the only well-established dietary treatment in IBD is exclusive enteral nutrition (EEN), which is used for induction of remission mostly in pediatric CD.5,6 Over the past 2 decades, several food-based exclusion diets have been suggested as potential treatments for CD and UC, some of which demonstrated promising efficacy signals such as the CD-TREAT (Crohn’s disease treatment with eating) diet and the CDED (Crohn’s disease exclusion diet).7-9 Nonetheless, current societal guidelines do not recommend the use of any solid food–based exclusion diet as a treatment option for the induction or maintenance of clinical remission in IBD.6“
Key findings:
Foods pertinent to a prudent dietary pattern (ie, fish, chicken, avocado, blueberries), foods high in pre- and probiotics, and certain food exclusion diets (eg, SCD) were primarily portrayed as beneficial.
Foods often associated with a Western dietary pattern, including processed foods, high-sugar foods and high-fat foods, red meat, and alcohol, were considered detrimental for disease outcomes in patients with IBD.
Neutral opinions were expressed about fiber and vegetables.
There was a higher video interaction rate and number of likes in patient-generated videos compared with videos from healthcare professionals.
Only 3% of all patient videos and 35% of videos from healthcare professionals cited any form of scientific evidence.
Problems with diet advice is that extensive dietary restrictions and adherence to extreme diets may lead to the development of disordered eating as well as nutrient deficiencies (nutritionist involvement is important to avoid this). In addition, reliance on unproven diets may lead some patients to forgo proven therapies.
My take: Though there are some overlapping advice in these videos, much of the dietary advice on YouTube (and elsewhere) is conflicting. In part, this reflects the lack of evidence-based dietary guidelines for IBD. Physicians should review information on dietary therapies at diagnosis and request that families contact them (or well-qualified nutritionists) when considering dietary modifications.
I was a little disappointed (aka first world problem) that this commentary appeared in the February print edition of The Journal of Pediatrics about 4 months after the publication of the analyzed study. This blog commented on this study in October: Disparities Are Abundant in Pediatrics -4 Studies on IBD, SUID, Specialty Referrals and in the NICU re: J Smith et al. J Pediatr 2023; 260: 113522.
“In this issue of The Journal, Smith et al report the results of an historical cohort analysis of 519 children and adolescents with newly diagnosed IBD (2013-2020)… Smith et al ask the question of whether the greater rate of complicated disease in Black patients is related more to delayed diagnosis or access to therapy rather than inherent race-based differences in response to treatment.”
Key points:
“In this study, Smith et al importantly identified no difference in initiating standard medical therapies based on race. Specifically, they report no difference in initial corticosteroid usage, time to initiation of maintenance therapy, or time to initiate antitumor necrosis factor therapy. In patients receiving biologics, both Black and White patients received similar loading doses and frequency of therapeutic drug monitoring.”
“Despite comparable disease presentation and approach to medical therapy in this study cohort,Black patients strikingly remained only one-half as likely to reach corticosteroid-free remission at 12 months compared with White patients (OR 0.52, 95% CI 0.3-0.9).”
” Black patients were less likely to be seen in gastroenterology specialty clinic for follow-up, more likely to present to the emergency department, and more likely to be hospitalized.”
“This study described poorer outcomes in Black patients despite similar treatments. However, the authors fail to arrive at a definitive answer as to why this is the case.”
My take: Black patients, even when offered similar IBD treatment, clearly experience inferior outcomes. While access and social determinants of health are important, there may be biological/phenotypic factors (eg. more aggressive disease) that are involved as well. More studies are needed. This editorial is a helpful review -the timing of the editorial in the print edition many months later, though, is a head-scratcher.
Unrelated topic: CDC COVID-19 Recommendation
The Centers for Disease Control and Prevention announced new isolation guidance for Covid-19 this week. At the start of the pandemic, people were recommended to stay home for 10 days after testing positive. At the height of the Omicron wave, that was revised to 5 days. This week, isolation time was revised to 24 hours without a fever and symptoms improving, which is similar to the recommendations for other illnesses.
This two part study involved a small open-label trial of combination curcumin-QingDai (CurQD) with 10 patients and a placebo-controlled trial with 42 patients with active ulcerative colitis (UC) over 8 weeks.
Background: “Curcumin and QingDai (QD, Indigo) are herbal compounds previously found to be effective in mild–moderate and moderate–severe ulcerative colitis (UC), respectively, but data on their use still are limited.” Curcumin has purported anti-inflammatory and antioxidant properties through downregulation of nuclear factor-kB, regulation the JAK/STAT pathways, and through its effects on the NLRP3 inflammasome. Qing Dai, also known as indigo naturalis, is a traditional Chinese medicine that has demonstrated efficacy in promoting recovery from colitis in animal models and prior human trials, potentially acting through activation of the aryl hydrocarbon receptor.
Methods: CurQD was administered as 3 capsules of 500 mg herbal extract dry powder QD (a total of 1.5 g) and 3 capsules of 500 mg dry powder curcumin (a total of 1.5 g)
Key findings:
Clinical response was observed in 85.7% vs 30.7% (P < .001), clinical remission in 14 of 28 (50%) vs 1 of 13 (8%; P = .01), a 50% calprotectin reduction in 46.4% vs 15.4% (P = .08), and endoscopic improvement in 75% vs 20% (P = .036) in the CurQD and placebo groups, respectively.
In the maintenance arm, 11/15 responders in the CurQD arm maintained remission for an additional 8 weeks with just curcumin alone.
The editorial (pg 235 ) notes the following:
The number of patients in the study is small and safety and effectiveness of these agents is not certain. Qing Dai has been associated with a rare risk of pulmonary arterial hypertension (especially with long-term use). Thus, further studies are needed.
“Although it may be preferrable to use these agents in combination with therapies with established efficacy, should the patients’ choice be to use alternative therapy as sole agents for treatment, it is important for us to continue to maintain a trusting physician-patient relationship to ensure that our patients are achieving the treatment targets they need to maximize long-term favorable outcomes, irrespective of the therapeutic agent of choice.”
My take: Curcumin (with combination of Qing Dai for induction) was superior to placebo in achieving meaningful clinical outcomes including clinical response, remission, calprotectin improvement and endoscopic improvement. For future studies, I would favor an active comparator like mesalamine rather than placebo.
In this retrospective study with 62 children (35 Crohn’s disease, 27 ulcerative colitis) with extensive and severe IBD that was refractory to various therapies, the authors examined the outcomes of combination therapies: the dual therapy included an anti-tumor necrosis factor agent and vedolizumab in 30 children (48%), anti-tumor necrosis factor and ustekinumab in 21 (34%) children, vedolizumab and ustekinumab in 8 (13%) children, and tofacitinib with a biologic in 3 (5%) children.
Key findings:
Clinical remission was observed in 21 (35%), 30 (50%), and 38 (63%) children at 3, 6, and 12 months, respectively.
Normalization of C-reactive protein and decrease in fecal calprotectin to <250 µg/g were achieved in 75% and 64%, respectively, at 12 months
Twenty-nine (47%) children sustained adverse events, 8 of which were regarded as serious and led to discontinuation of therapy in 6.
Among the 43% that were receiving steroids at the start of dual therapy, twenty (74%) of them could be successfully weaned within 3 months after the initiation of dual therapy.
Only 2 of 23 (8.7%) had endoscopic healing
My take (borrowed partly from authors):
“Dual biologic therapy may be effective in children with refractory IBD. The potential efficacy should be weighed against the risk of serious adverse events” and affordability.
“There are currently no data for identifying the patients that are more likely to benefit from dual therapy….The ideal selection of dual biologic regimens remains to be determined.”
This study examined more than 13,000 patients enrolled in a prospective cohort study from the British Association of Dermatologists Biologics and Immunomodulators Register for adults treated with biologics for plaque psoriasis.
Key findings:
A total of 273 exposures (1%) were associated with paradoxical eczema.
The adjusted incidence rates were 0.94 per 100 000 person-years for TNF inhibitors, 0.80 per 100 000 person-years for IL-12/23 inhibitors, and 0.56 per 100 000 person-years for IL-23 inhibitors. IL-23 inhibitors were associated with a lower risk of paradoxical eczema (hazard ratio [HR], 0.39)
My take (from authors): The overall incidence of paradoxical eczema was low in biologic-treated patients with psoriasis. The risk was lowest in patients receiving IL-23 inhibitors. Increasing age, female sex, and history of AD or hay fever were associated with higher risk of paradoxical eczema.
Gastroenterol 2024; 166: 87. Open Access! Spotlight (1 page summary)
Key recommendations
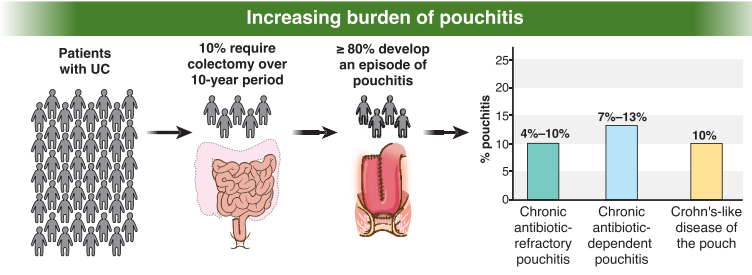
AGA recommends metronidazole and/or ciprofloxacin as preferred treatment of pouchitis with duration of treatment 2-4 weeks.
For Crohn’s-like disease of the pouch, AGA guideline recommends using either ileal-release budesonide or advanced immunosuppressive agents (eg. Biological therapies and small molecule therapies)
“In patients with cuffitis, topical therapies should be the first-line therapy, such as mesalamine suppositories, corticosteroid suppositories, or corticosteroid ointment applied directly to the cuff. Biological therapies and small molecule therapies are recommended in refractory cases