In this retrospective study of 41 adults with history of ileal pouch-anal anastomosis (IPAA) for ulcerative colitis (UC), the authors evaluated the clinical response (subjective judgement of provider) to chronic vancomycin therapy (125 mg twice a day).
Key findings:
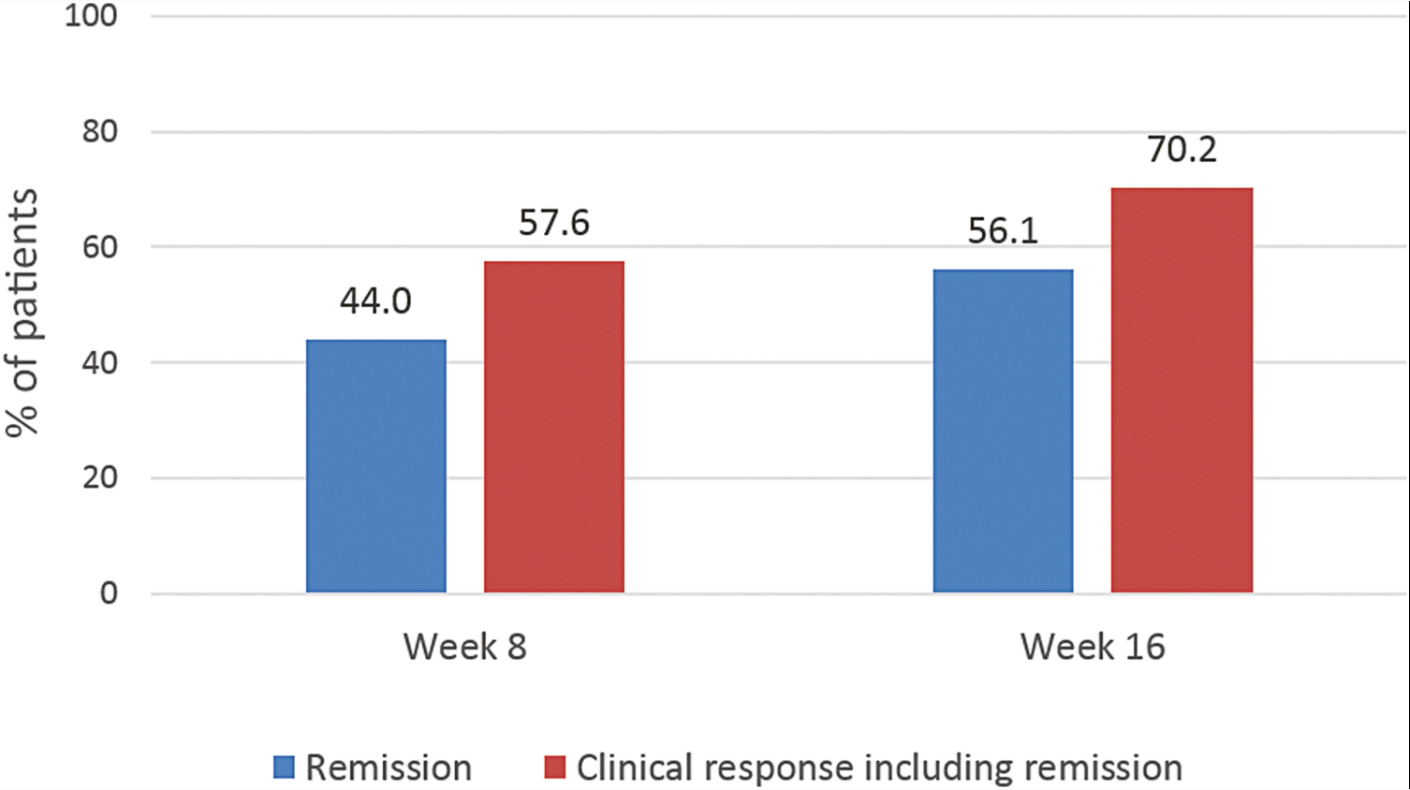
At 4 weeks, 21 (51%) of patients had a clinical response. 16 of these patients maintained a clinical response at 3 and 6 months (remained on treatment).
6 additional patients demonstrated a later response. In total 22 (54%) were considered clinical responders at 3 and 6 months.
The mean number of antibiotics utilized prior to vancomycin was 4, including ciprofloxacin, metronidazole, levofloxacin, rifaximin, sulamethoxazole-trimetoprim, amoxicillin, and amoxicillin-clavulanic acid
My take: Since vancomycin has poor enteral absorption, it’s side effect profile is very favorable. More prospective and objective data is needed; however, vancomycin’s high cost will likely limit frequent use.
Methods: In patients (n=99) with Rome IV–defined non-constipated IBS, outcomes after randomization to one of three diets were compared. The “traditional dietary advice” group: “Its principles include adopting healthy, sensible eating patterns such as having regular meals, never eating too little/too much, maintaining adequate hydration, and reducing the intake of (1) alcohol/caffeine/fizzy drinks, (2) fatty/spicy/processed foods, (3) fresh fruit to a maximum of 3 per day, (4) fiber and other commonly consumed gas-producing foods (eg, beans, bread, sweeteners, etc), and (5) addressing any perceived food intolerances (eg, dairy).” (Link: National Institute for Health and Care Excellenceadvice on IBS mgt). The Gluten-Free diet allowed for cross-contamination. All patients had specialist dietary counseling.
Key findings:
All three diets resulted in improvement. The primary end point of ≥50-point reduction in IBS-SSS was met by 42% (n = 14/33) undertaking TDA, 55% (n = 18/33) for LFD, and 58% (n = 19/33) for GFD (P = .43)
Alterations in stool dysbiosis index were similar across the diets, with 22%–29% showing reduced dysbiosis
“The pragmatic study design, whereby the responsibility was left on patients to undertake the diets following appropriate education, means our findings can be generalized”
My take: All three diet approaches would be appropriate to reduce IBS symptoms, thought the TDA is the easiest for patients.
Thank you to those who have helped me this past year with this blog –colleagues, friends and family. Wishing all of you a good 2023. Here are some of my favorite posts from this past year:
This article has 91 authors! Using Delphi surveys, the authors recommend the following:
“EGID” was the preferred umbrella term for disorders of gastrointestinal (GI) tract eosinophilic inflammation in the absence of secondary causes
Involved GI tract segments will be named specifically and use an “Eo” abbreviation convention: eosinophilic gastritis (now abbreviated EoG), eosinophilic enteritis (EoN), and eosinophilic colitis (EoC)
For EoN, “it is desirable, but not required, to name specific locations of small bowel involvement, if these are known…The abbreviation for eosinophilic duodenitis should be “EoD”… for eosinophilic jejunitis should be “EoJ”….eosinophilic ileitis should be “EoI”
The term “eosinophilic gastroenteritis” is no longer preferred as the overall name (but can be used to indicate involvement of both the stomach and small bowel)
When >2 GI tract areas are involved, the name should reflect all of the involved areas
Compared with WD1 (typical Western Diet), PB2 (Plant-based diet 2) was associated with lower odds of active symptoms for CD (odds ratio [OR], 0.32
PB1 (Plant-based diet 1) was associated with lower odds of active symptoms for participants with UC (OR, 0.45; 95% CI, 0.23-0.90) but not for participants with CD (OR, 0.95
Diet PB1 (“Plant-based Diet 1”) was characterized by much higher intake of fruits, vegetables, plant-based proteins, and cooked grains than most other dietary clusters. There was low water intake in favor of juices and other beverages. There was otherwise average intake of added fats and oils, sugars, seafood, and dairy products, and modest intake of meats, eggs, mixed grains, and breads.
Diet PB2 (“Plant-based Diet 2”) was characterized by high intake of fruits, vegetables, plant proteins, and cooked grains and low intake of animal proteins (especially red and cured meats), added fats, sweetened beverages, sweet bakery products, other desserts, eggs, and breads. There was also a reduction of other beverages in favor of water. There was otherwise an average intake of seafood and dairy products.
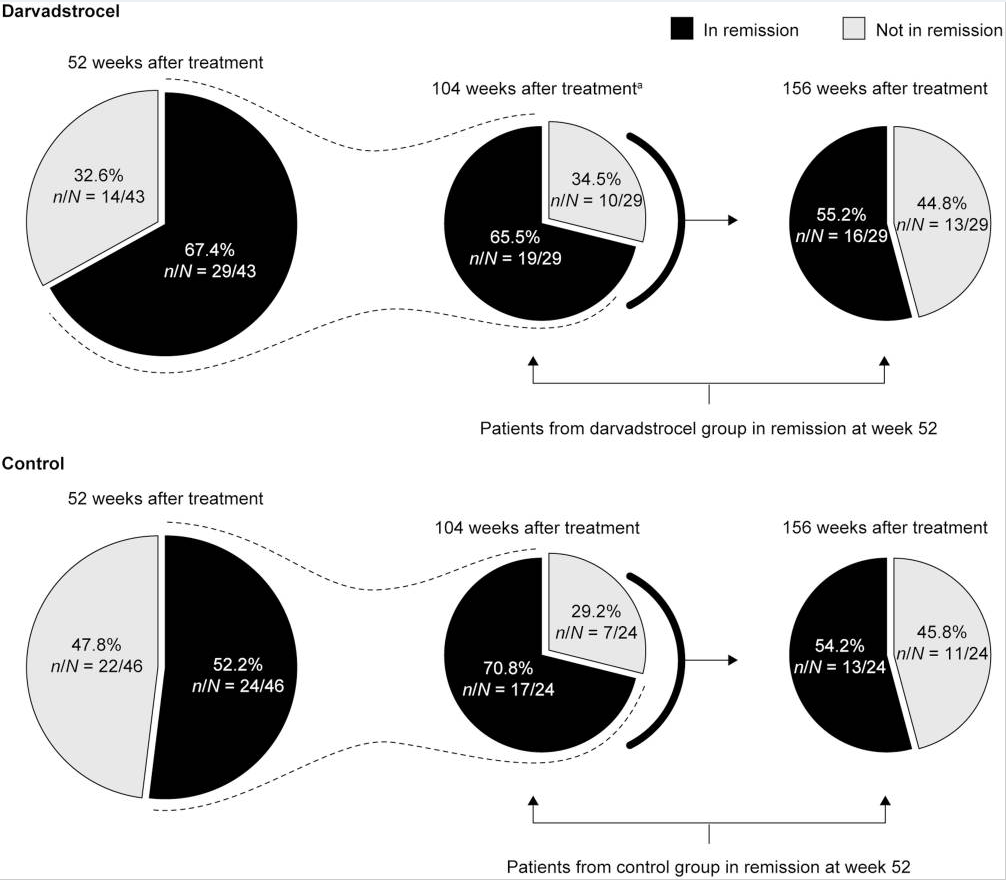
Background: The current chart review study evaluated the longer-term effectiveness and safety of darvadstrocel (expanded allogeneic adipose-derived mesenchymal stem cells).; n=43 treated patient and n=46 controls.
Key findings:
At 52, 104, and 156 weeks posttreatment, clinical remission was observed in 29 (67.4%) of 43, 23 (53.5%) of 43, and 23 (53.5%) of 43 darvadstrocel-treated patients, compared with 24 (52.2%) of 46, 20 (43.5%) of 46, and 21 (45.7%) of 46 control subjects, respectively.
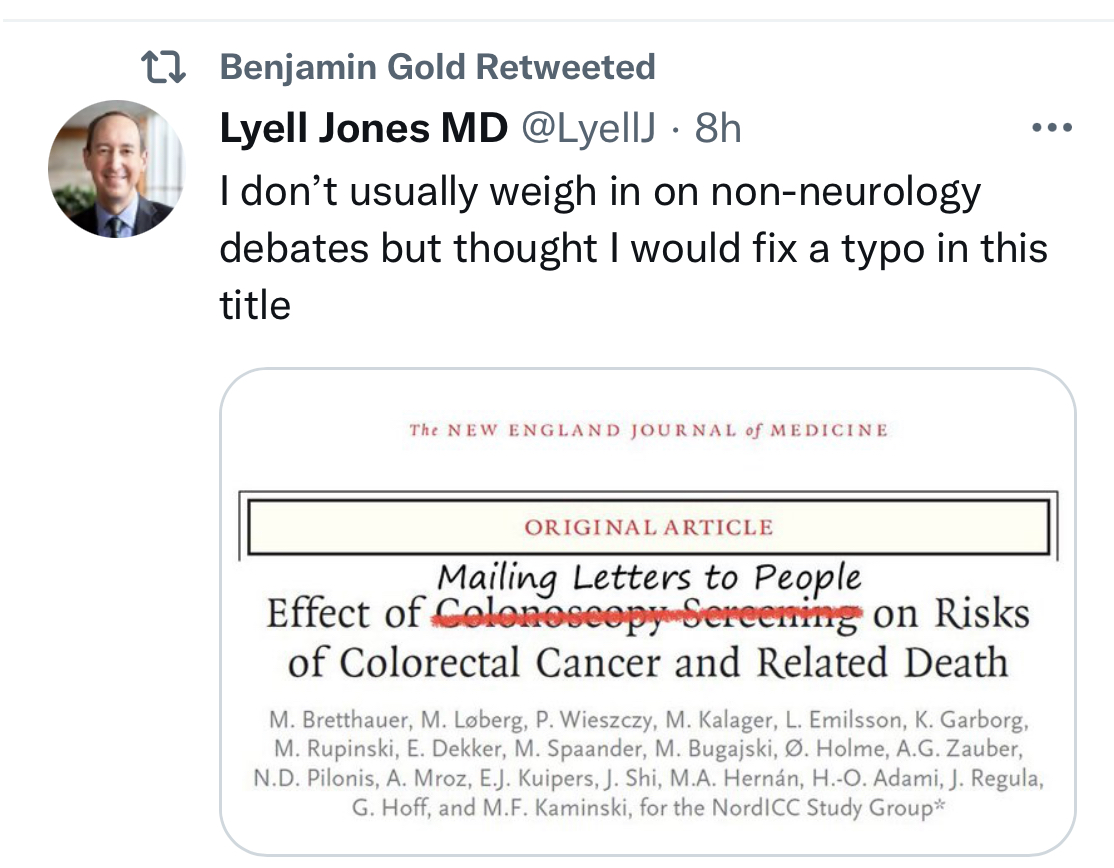
A widely covered news story in October 2022 was the disappointing results/modest benefits of a colonoscopy screening study. This study actually supports the use of colonoscopy to reduce colorectal cancer deaths but shows that typical screening programs may not work well if patients don’t show up for the test.
Methods: This was “a pragmatic, randomized trial involving presumptively healthy men and women 55 to 64 years of age drawn from population registries in Poland, Norway, Sweden, and the Netherlands between 2009 and 2014. The participants were randomly assigned in a 1:2 ratio either to receive an invitation to undergo a single screening colonoscopy (the invited group) or to receive no invitation or screening (the usual-care group).”
There were 84,585 participants in Poland, Norway, and Sweden — 28,220 in the invited group,
Key findings:
Only 11,843 (42.0%) in the invited group underwent colonoscopy screening
During a median follow-up of 10 years, 259 cases of colorectal cancer were diagnosed in the invited group as compared with 622 cases in the usual-care group
The risk of colorectal cancer at 10 years was 0.98% in the invited group and 1.20% in the usual-care group, a risk reduction of 18%
The risk of death from colorectal cancer was 0.28% in the invited group and 0.31% in the usual-care group (risk ratio, 0.90; 95% CI, 0.64 to 1.16)
The risk of death from any cause was 11.03% in the invited group and 11.04% in the usual-care group
If all invited participants had received a colonoscopy, the authors estimate the risk of colorectal cancer would have decreased from 1.22% to 0.84% and the risk of colorectal cancer death would have been reduced from 0.3% to 0.15% (a 50% drop).
My take: Colonoscopy as a screening tool only works if it is performed. Given the low response rate for screening, other tools like an annual fecal immunochemical test (FIT) need to be considered as alternatives.
Background: NSAIDs are well-known to cause gastrointestinal injury. While single center studies have suggested that NSAIDs are associated with increased IBD flares, a systemic review of 18 studies found no consistent association between NSAIDs and IBD exacerbation.
This study included 15,705 (44.8%) and 19,326 (55.2%) IBD patients with and without an NSAID exposure.
Key findings:
Findings from a Cox proportional hazards model suggest an association between NSAIDs and IBD exacerbation (HR 1.24; 95%CI 1.16-1.33)
However, the likelihood of an IBD exacerbation in the NSAID exposed arm preceding NSAID exposure was similar (HR 1.30; 95%CI 1.21-1.39).
Those who received NSAIDs were already at increased risk of experiencing a disease flare. And the prior event rate ratio for IBD exacerbation, as determined by dividing the adjusted HR after NSAID exposure by the adjusted HR for pre-NSAID exposure, was 0.95 (95% CI, 0.89 – 1.01).
“A self-controlled case series analysis of 3,968 patients who had both an NSAID exposure and IBD exacerbation demonstrated similar exacerbation rates in the 1-year preceding exposure, 2-6 weeks post-exposure, and 6-weeks to 6-months post-exposure, but higher incidence 0-2 weeks post-exposure, suggesting potential confounding by reverse causality.” The self-controlled part of the study allowed patients to serve as their own controls which allowed adjustment for many factors that are difficult to control with retrospective studies.
75% of patients with IBD who were prescribed an NSAID did not have an IBD exacerbation during a mean of 5.9 years of follow-up
NSAIDs were commonly used: 36.5% of patients with IBD had received at least one NSAID prescription
NSAIDs use was prescribed more frequently in patients with immune targeted therapy (likely a marker for moderate to severe disease)
Discussion points:
The estimated prior event ratio of 0.95 suggests that the risk of IBD flares in NSAID-exposed patients preceded the use of NSAIDs. The risk of IBD exacerbation did not increase in the 2 weeks to 6 months after NSAID exposure.
The overall association of increased IBD flare is likely related to reverse causation. Patients may take NSAIDs due to arthropathy or other symptoms that may be an early manifestation of a flare.
My take: This study challenges the prevailing view that NSAID use worsen inflammatory bowel disease; it is more likely that IBD exacerbations are due to underlying risk from more severe disease and residual confounding/reverse causality. The study provides reassurance that short-duration use is likely to be well-tolerated in most patients with IBD.
Methods: This was “a randomised, double-blind, parallel-group, active-comparator, phase 3b trial (SEAVUE) at 121 hospitals or private practices in 18 countries. We included biologic-naive patients aged 18 years or older with moderately to severely active Crohn’s…Eligible patients were randomly assigned (1:1; via an interactive web response system) to receive ustekinumab (approximately 6 mg/kg intravenously on day 0, then 90 mg subcutaneously once every 8 weeks) or adalimumab (160 mg on day 0, 80 mg at 2 weeks, then 40 mg once every 2 weeks, subcutaneously) through week 56. Study treatments were administered as monotherapy and without dose modifications.”
386 patients were enrolled.
Key findings:
29 (15%) of 191 patients in the ustekinumab group and 46 (24%) of 195 in the adalimumab group discontinued study treatment before week 52
At week 52, 124 (65%) of 191 patients in the ustekinumab group versus 119 (61%) of 195 in the adalimumab group were in clinical remission (CDAI <150)
Endoscopic remission at week 52: ustekinumab 29% and for adalimumab 29%
Endoscopic response at week 52: ustekinumab 42%and for adalimumab 37%
Rapid onset of clinical response was seen with both therapies with improvement noted as early as week 2 assessment
Antidrug antibodies were less frequent with ustekinumab compared to adalimumab: 2% vs 74%.
Infections were reported in 65 (34%) of ustekinumab group compared to 79 (41%) of adalimumab group. Serious infections were reported in four (2%) of 191 patients in the ustekinumab group and five (3%) of 195 in the adalimumab group.
No deaths occurred through week 52 of the study.
My take:
Both medications had a high similar response rate. Ustekinumab had fewer patients discontinue medication and lower immunogenicity which could improve efficacy/duration of response in an extended study.
It is good to see a well-designed head-to-head study rather than a placebo-control arm. Placebo-based studies are hard to justify given the availability of multiple effective agents.
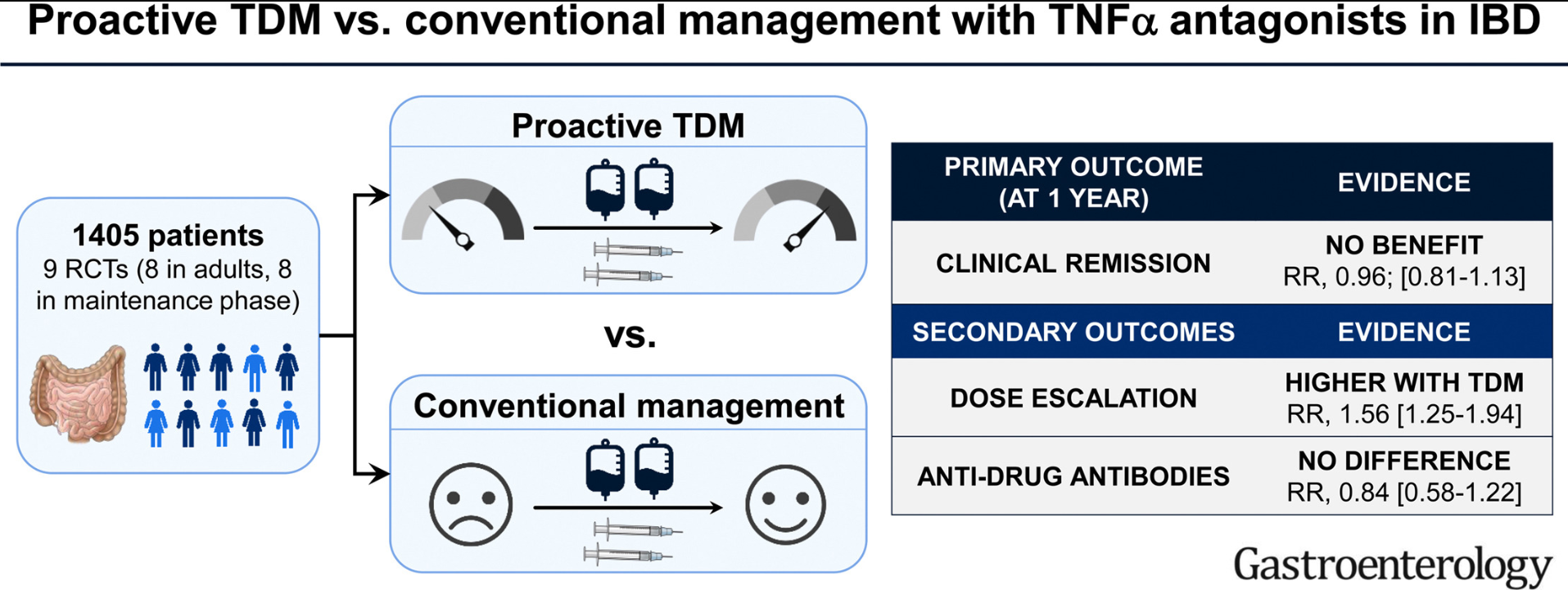
On meta-analysis of 9 RCTs (8 RCTs in adults, and focusing on maintenance phase), there was no significant difference in the risk of failing to maintain clinical remission in patients who underwent proactive TDM (267/709; 38%) vs conventional management (292/696; 42%) (relative risk [RR], 0.96)
The discussion in this paper makes some important points, as there are some populations in which proactive TDM is more likely to be beneficial.
Pediatrics:
“The impact of proactive TDM in pediatric patients also merits further consideration. This concept may be particularly important in pediatrics due to the variability in size of patients, which may not be adequately addressed by weight-based dosing.33 This is especially important in younger children, where it has been shown that standard TNFα antagonist regimens and trough levels may not be applicable in this age group, and may require more frequent escalation of therapy.34,35 In the PAILOT trial, proactive TDM in children with clinical response to adalimumab was associated with higher rates of maintaining sustained corticosteroid-free clinical remission at all visits from week 8–72, compared with reactive TDM in which physicians were informed of trough concentration only after loss of response.”
Induction Dosing (Adults and Children):
“It is possible that the early measurement of biologic drug concentrations, to identify patients who may have accelerated clearance, and optimization of a subset of these patients early in the course of therapy may offer benefit.1,30 …Ongoing trials such as OPTIMIZE (NCT04835506) and TITRATE (NCT03937609) in which infliximab is optimized during the induction phase through a pharmacokinetic dashboard in patients with Crohn’s disease and acute severe ulcerative colitis will shed further light on this.”
My take: So far, studies in adults have not shown that proactive therapeutic drug monitoring has been effective in improving clinical outcomes. This may change particularly if studies focus on patients on monotherapy who are at increased risk of subtherapeutic levels. No matter what happens in adults, there is sufficient data showing that proactive therapeutic drug monitoring is essential in children. This is especially important as ‘routine” dosing of infliximab in children may be subtherapeutic in nearly 80%.